Ann Surg Treat Res.
2015 Sep;89(3):111-116. 10.4174/astr.2015.89.3.111.
Minimally invasive parathyroidectomy with or without intraoperative parathyroid hormone for primary hyperparathyroidism
- Affiliations
-
- 1Department of Surgery, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Korea.
- 2Department of Anesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. ylee@amc.seoul.kr
- KMID: 2166929
- DOI: http://doi.org/10.4174/astr.2015.89.3.111
Abstract
- PURPOSE
The improvement of intraoperative parathyroid hormone (IOPTH) assay and localization studies has enabled a minimally invasive parathyroidectomy (MIP) in primary hyperparathyroidism (pHPT). The aim of this study is to analyze the demographics, clinical presentations, and surgical outcomes of the pHPT patients who received surgical management with versus without IOPTH.
METHODS
Analysis of a database was performed on 53 patients who underwent parathyroidectomy for pHPT from 2004 to 2013. Preoperative localization was done by both sestamibi scan and ultrasonography. We divided the patients into two groups (without IOPTH versus with IOPTH) and analyzed the surgical outcomes statistically between two groups.
RESULTS
The concordance rate of Technetium 99m sestamibi scan and ultrasonography was 73.6% and 90.6%, respectively. The overall cure rate of group 1 (without IOPTH) was 94.9% and that of group 2 (with IOPTH) was 100%. The decline of PTH at postoperative 5 minutes and 10 minutes was 75.2% +/- 14.9% and 84.9% +/- 8.6% in cured patients. On the other hand, that of noncured patients at 5 minutes and 10 minutes was 17.2% +/- 9.7% and 8.2% +/- 2.2%. There was a significant difference in the drop rate of IOPTH between cured and persistent patients (P < 0.01). Pathological examination showed adenoma in 41 of 53 patients (77.4%) and hyperplasia in 10 of 53 patients (18.9%).
CONCLUSION
Even though the localization studies were successful, IOPTH monitoring is essential to avoid a surgical failure in MIP.
Keyword
MeSH Terms
Figure
-
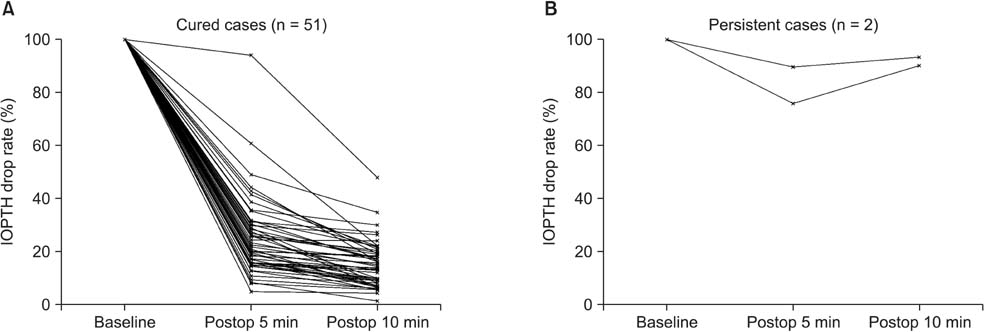
Fig. 1 Results of intraoperative parathyroid hormone in cured patients (A) and in persistent patients (B). IOPTH, intraoperative parathyroid hormone; Postop, postoperative.
Reference
-
1. Marcocci C, Cetani F. Clinical practice: primary hyperparathyroidism. N Engl J Med. 2011; 365:2389–2397.2. Lee SW, Park H, Shin JM, Lee YM, Park JH, Koh YW, et al. Clinical analysis of parathyroid adenoma with primary hyperparathyroidism. Korean J Otolaryngol-Head Neck Surg. 2006; 49:72–78.3. Lundgren E, Lind L, Palmer M, Jakobsson S, Ljunghall S, Rastad J. Increased cardiovascular mortality and normalized serum calcium in patients with mild hypercalcemia followed up for 25 years. Surgery. 2001; 130:978–985.4. Ollila DW, Caudle AS, Cance WG, Kim HJ, Cusack JC, Swasey JE, et al. Successful minimally invasive parathyroidectomy for primary hyperparathyroidism without using intraoperative parathyroid hormone assays. Am J Surg. 2006; 191:52–56.5. Bilezikian JP, Khan AA, Potts JT Jr. Third International Workshop on the Management of Asymptomatic Primary Hyperthyroidism. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the third international workshop. J Clin Endocrinol Metab. 2009; 94:335–339.6. Phillips IJ, Kurzawinski TR, Honour JW. Potential pitfalls in intraoperative parathyroid hormone measurements during parathyroid surgery. Ann Clin Biochem. 2005; 42(Pt 6):453–458.7. Schneider DF, Mazeh H, Sippel RS, Chen H. Is minimally invasive parathyroidectomy associated with greater recurrence compared to bilateral exploration? Analysis of more than 1,000 cases. Surgery. 2012; 152:1008–1015.8. Sebag F, Shen W, Brunaud L, Kebebew E, Duh QY, Clark OH. Intraoperative parathyroid hormone assay and parathyroid reoperations. Surgery. 2003; 134:1049–1055.9. Chen H, Mack E, Starling JR. A comprehensive evaluation of perioperative adjuncts during minimally invasive parathyroidectomy: which is most reliable? Ann Surg. 2005; 242:375–380.10. Mihai R, Palazzo FF, Gleeson FV, Sadler GP. Minimally invasive parathyroidectomy without intraoperative parathyroid hormone monitoring in patients with primary hyperparathyroidism. Br J Surg. 2007; 94:42–47.11. Pang T, Stalberg P, Sidhu S, Sywak M, Wilkinson M, Reeve TS, et al. Minimally invasive parathyroidectomy using the lateral focused mini-incision technique without intraoperative parathyroid hormone monitoring. Br J Surg. 2007; 94:315–319.12. Augustine MM, Bravo PE, Zeiger MA. Surgical treatment of primary hyperparathyroidism. Endocr Pract. 2011; 17:Suppl 1. 75–82.13. Low RA, Katz AD. Parathyroidectomy via bilateral cervical exploration: a retrospective review of 866 cases. Head Neck. 1998; 20:583–587.14. Jacobson SR, van Heerden JA, Farley DR, Grant CS, Thompson GB, Mullan BP, et al. Focused cervical exploration for primary hyperparathyroidism without intraoperative parathyroid hormone monitoring or use of the gamma probe. World J Surg. 2004; 28:1127–1131.15. Udelsman R, Lin Z, Donovan P. The superiority of minimally invasive parathyroidectomy based on 1650 consecutive patients with primary hyperparathyroidism. Ann Surg. 2011; 253:585–591.16. Miccoli P, Bendinelli C, Berti P, Vignali E, Pinchera A, Marcocci C. Video-assisted versus conventional parathyroidectomy in primary hyperparathyroidism: a prospective randomized study. Surgery. 1999; 126:1117–1121.17. Hughes DT, Miller BS, Doherty GM, Gauger PG. Intraoperative parathyroid hormone monitoring in patients with recognized multiglandular primary hyperparathyroidism. World J Surg. 2011; 35:336–341.18. Rajaei MH, Oltmann SC, Adkisson CD, Elfenbein DM, Chen H, Carty SE, et al. Is intraoperative parathyroid hormone monitoring necessary with ipsilateral parathyroid gland visualization during anticipated unilateral exploration for primary hyperparathyroidism: a two-institution analysis of more than 2,000 patients. Surgery. 2014; 156:760–766.19. Nussbaum SR, Thompson AR, Hutcheson KA, Gaz RD, Wang CA. Intraoperative measurement of parathyroid hormone in the surgical management of hyperparathyroidism. Surgery. 1988; 104:1121–1127.20. Miura D, Wada N, Arici C, Morita E, Duh QY, Clark OH. Does intraoperative quick parathyroid hormone assay improve the results of parathyroidectomy? World J Surg. 2002; 26:926–930.21. Carneiro DM, Solorzano CC, Nader MC, Ramirez M, Irvin GL 3rd. Comparison of intraoperative iPTH assay (QPTH) criteria in guiding parathyroidectomy: which criterion is the most accurate? Surgery. 2003; 134:973–979.22. Barczynski M, Konturek A, Hubalewska-Dydejczyk A, Cichon S, Nowak W. Evaluation of Halle, Miami, Rome, and Vienna intraoperative iPTH assay criteria in guiding minimally invasive parathyroidectomy. Langenbecks Arch Surg. 2009; 394:843–849.23. Irvin GL 3rd, Carneiro DM, Solorzano CC. Progress in the operative management of sporadic primary hyperparathyroidism over 34 years. Ann Surg. 2004; 239:704–708.24. Khan A, Bilezikian J. Primary hyperparathyroidism: pathophysiology and impact on bone. CMAJ. 2000; 163:184–187.25. Adkisson CD, Koonce SL, Heckman MG, Thomas CS, Harris AS, Casler JD. Predictors of accuracy in preoperative parathyroid adenoma localization using ultrasound and Tc-99m-Sestamibi: a 4-quadrant analysis. Am J Otolaryngol. 2013; 34:508–516.26. Prasannan S, Davies G, Bochner M, Kollias J, Malycha P. Minimally invasive parathyroidectomy using surgeon-performed ultrasound and sestamibi. ANZ J Surg. 2007; 77:774–777.27. Chapuis Y, Fulla Y, Bonnichon P, Tarla E, Abboud B, Pitre J, et al. Values of ultrasonography, sestamibi scintigraphy, and intraoperative measurement of 1-84 PTH for unilateral neck exploration of primary hyperparathyroidism. World J Surg. 1996; 20:835–839.28. Chiu B, Sturgeon C, Angelos P. What is the link between nonlocalizing sestamibi scans, multigland disease, and persistent hypercalcemia? A study of 401 consecutive patients undergoing parathyroidectomy. Surgery. 2006; 140:418–422.29. Strichartz SD, Giuliano AE. The operative management of coexisting thyroid and parathyroid disease. Arch Surg. 1990; 125:1327–1331.30. Morita SY, Somervell H, Umbricht CB, Dackiw AP, Zeiger MA. Evaluation for concomitant thyroid nodules and primary hyperparathyroidism in patients undergoing parathyroidectomy or thyroidectomy. Surgery. 2008; 144:862–866.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative Parathyroid Hormone Monitoring in the Surgical Management of Sporadic Primary Hyperparathyroidism
- Role and Recent Trend of Intraoperative Parathyroid Hormone Monitoring During Parathyroidectomy in Patients With Primary Hyperparathyroidism
- Usefulness of Intraoperative Parathyroid Hormone Assay in Minimally Invasive Surgery
- Minimally Invasive Parathyroidectomy without an Intraoperative i-PTH Test for Patients with Primary Hyperparathyroidism
- Primary Hyperparathyroidism in Recurrent Urolithiasis: 1 Case
