Cancer Res Treat.
2010 Mar;42(1):30-36.
Predictors of Axillary Lymph Node Metastases (ALNM) in a Korean Population with T1-2 Breast Carcinoma: Triple Negative Breast Cancer has a High Incidence of ALNM Irrespective of the Tumor Size
- Affiliations
-
- 1Department of Radiation Oncology, St. Vincent's Hospital, The Catholic University College of Medicine, Suwon, Korea. kimandre@catholic.ac.kr
- 2Department of Surgical Oncology, St. Vincent's Hospital, The Catholic University College of Medicine, Suwon, Korea.
- 3Department of Medical Oncology, St. Vincent's Hospital, The Catholic University College of Medicine, Suwon, Korea.
Abstract
- PURPOSE
We estimated the likelihood of breast cancer patients having axillary lymph node metastases (ALNM) based on a variety of clinical and pathologic factors. MATERIALS AND METHODS: Three hundred sixty-one breast cancer patients without distant metastases and who underwent breast conserving surgery and axillary lymph node dissection (ALND) (level I and II) or modified radical mastectomy (MRM) were identified, and we retrospectively reviewed their pathology records and treatment charts. RESULTS: Positive axillary lymph nodes were detected in 104 patients for an overall incidence of 28.8%: 2 patients (5%) with T1a tumor, 5 (9.2%) with T1b tumor, 24 (21.8%) with T1c tumor and 73 (44.2%) with T2 tumor. On the multivariate analysis, an increased tumor size (adjusted OR=11.87, p=0.02), the presence of lymphovascular invasion (adjusted OR=7.41, p<0.01), a triple negative profile (ER/PR-, Her2-) (adjusted OR=2.09, p=0.04) and a palpable mass at the time of diagnosis (adjusted OR=2.31, p=0.03) were all significant independent factors for positive ALNM. CONCLUSION: In our study, the tumor size, the presence of lymphovascular invasion, a triple negative profile and a palpable mass were the independent predictive factors for ALNM. The tumor size was the strongest predictor of ALNM. Thus, the exact estimation of the extent of tumor is necessary for clinicians to optimize the patients' care. Patients with a triple negative profile have a high incidence of ALNM irrespective of the tumor size.
Keyword
MeSH Terms
Figure
-
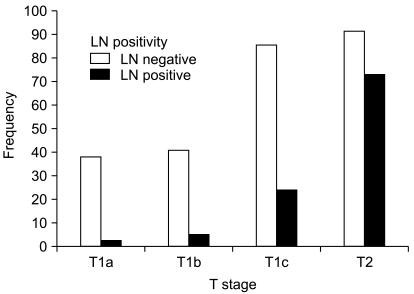
Fig. 1 The frequency of nodal positivity according to the tumor size. Positive axillary lymph nodes were detected in 104 patients for an overall incidence of 28.8%: 2 patients (5%) with T1a; 5 (9.2%) with T1b; 24 (21.8%) with T1c; and 73 (44.2%) with T2. As the tumor size increased, the frequency of positive axillary nodes were also increased (p<0.001).
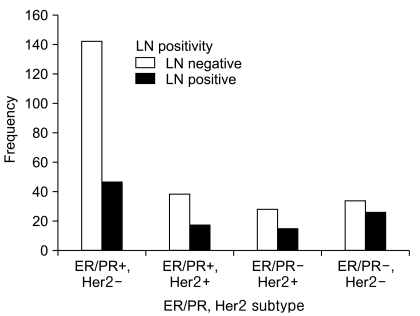
Fig. 2 The frequency of the tumor subtypes according to the ER, PR and Her2 statuses. The ER/PR+,Her2- profile was the most common subtype (n=189). Patients with triple negative (ER/PR-,Her2-) profile have a significantly increased probability of ALNM than patients with ER/PR+,Her2- profile (p=0.006).
Reference
-
1. Rosen PP, Groshen S, Kinne DW, Norton L. Factors influencing prognosis in node-negative breast carcinoma: analysis of 767 T1N0M0/T2N0M0 patients with long-term follow-up. J Clin Oncol. 1993; 11:2090–2100. PMID: 8229123.
Article2. Fisher B, Bauer M, Wickerham DL, Redmond CK, Fisher ER, Cruz AB, et al. Relation of number of positive axillary nodes to the prognosis of patients with primary breast cancer: an NASABP update. Cancer. 1983; 52:1551–1557. PMID: 6352003.3. Consensus statement treatment of early-stage breast cancer. National Institutes of Health Consensus Development Panel. J Natl Cancer Inst Monogr. 1992; 11:1–5.4. NIH Consensus Conference, Treatment of early-stage breast cancer. JAMA. 1991; 265:391–395. PMID: 1984541.5. Davies GC, Millis RR, Hayward JL. Assessment of axillary lymph node status. Ann Surg. 1980; 192:148–151. PMID: 7406568.
Article6. Kang HS, Noh DY, Youn YK, Oh SK, Choe KJ. The predictors of axillary node metastasis in 2 cm or less breast cancer univariate and multivaritate analysis. J Korean Breast Cancer Soc. 1999; 2:7–13.
Article7. Nemoto T, Vana J, Bedwani RN, Baker HW, McGregor FH, Murphy GP. Management and survival of female breast cancer: results of a national survey by the American college of surgeons. Cancer. 1980; 45:2917–2924. PMID: 7388735.
Article8. Ernst MF, Voogd AC, Balder W, Klinkenbijl JH, Roukema JA. Early and late morbidity associated with axillary levels I-III dissection in breast cancer. J Surg Oncol. 2002; 79:151–155. PMID: 11870664.
Article9. Mansel RE, Fallowfield L, Kissin M, Goyal A, Newcombe RG, Dixon JM, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC Trial. J Natl Cancer Inst. 2006; 98:599–609. PMID: 16670385.
Article10. Frederick LG, David LP, Irvin DF, April F, Charles MB, Daniel GH, et al. AJCC Cancer Staging Manual/American Joint Committee on Cancer. Breast. 2002. 6th ed. Philadelphia: Lippincott Williams & Wilkins;p. 223–240.11. Tinnemans JG, Wobbes T, Holland R, Hendriks JH, Van der Sluis RF, De Boer HH. Treatment and survival of female patients with nonpalpable breast carcinoma. Ann Surg. 1989; 209:249–253. PMID: 2537064.
Article12. Silverstein MJ, Skinner KA, Lomis TJ. Predicting axillary nodal positivity in 2282 patients with breast carcinoma. World J Surg. 2001; 25:767–772. PMID: 11376414.
Article13. Kambouris AA. Axillary node metastases in relation to size and location of breast cancers: analysis of 147 patients. Am Surg. 1996; 62:519–524. PMID: 8651544.14. Fein DA, Fowble BL, Hanlon AL, Hooks MA, Hoffman JP, Sigurdson ER, et al. Identification of women with T1-T2 breast cancer at low risk of positive axillary nodes. J Surg Oncol. 1997; 65:34–39. PMID: 9179265.
Article15. Cetinas SK, Kurt M, Ozkan L, Engin K, Gökgöz S, Tasdelen I. Factors influencing axillary node metastasis in breast cancer. Tumori. 2006; 92:416–422. PMID: 17168435.
Article16. Jonjic N, Mustac E, Dekanic A, Marijic B, Gaspar B, Kolic I, et al. Predicting sentinel lymph node metastases in infiltrating breast carcinoma with vascular invasion. Int J Surg Pathol. 2006; 14:306–311. PMID: 17041193.
Article17. Bevilacqua J, Cody H 3rd, MacDonald KA, Tan LK, Borgen PI, Van Zee KJ. A prospective validated model for predicting axillary node metastases based on 2000 sentinel node procedures: the role of tumor location [corrected]. Eur J Surg Oncol. 2002; 28:490–500. PMID: 12217300.18. Colleoni M, Rotmensz N, Maisonneuve P, Sonzogni A, Pruneri G, Casadio C, et al. Prognostic role of the extent of peritumoral vascular invasion in operable breast cancer. Ann Oncol. 2007; 18:1632–1640. PMID: 17716986.
Article19. Carey LA, Perou CM, Livasy CA, Dressler LG, Cowan D, Conway K, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006; 295:2492–2502. PMID: 16757721.
Article20. Onitilo AA, Engel JM, Greenlee RT, Mukesh BN. Breast cancer subtypes based on ER/PR and Her2 expression: comparison of clinicopathologic features and survival. Clin Med Res. 2009; 7:4–13. PMID: 19574486.
Article21. Bader AA, Tio J, Petru E, Bühner M, Pfahlberg A, Volkholz H, et al. T1 breast cancer: identification of patients at low risk of axillary lymph node metastases. Breast Cancer Res Treat. 2002; 76:11–17. PMID: 12408371.
Article22. Chua B, Ung O, Taylor R, Boyages J. Frequency and predictors of axillary lymph node metastases in invasive breast cancer. ANZ J Surg. 2001; 71:723–728. PMID: 11906387.
Article23. Martelli G, Boracchi P, De Palo M, Pilotti S, Oriana S, Zucali R, et al. A randomized trial comparing axillary dissection to no axillary dissection in older patients with T1N0 breast cancer: results after 5 years of follow-up. Ann Surg. 2005; 242:1–6. PMID: 15973094.24. Kim HJ, Chang MA, Hong SJ, Lee JS, Jung MS, Kim MJ, et al. Result of sentinel lymph node biopsy using radioisotope in clinically lymph node negative breast cancer. J Breast Cancer. 2007; 10:141–146.
Article25. Harden SP, Neal AJ, Al-Nasiri N, Ashley S, Querci della Rovere G. Predicting axillary lymph node metastases in patients with T1 infiltrating ductal carcinoma of the breast. Breast. 2001; 10:155–159. PMID: 14965577.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Predictors of Axillary Lymph Node Metastases in Patients with T1 Breast Cancer
- The Predictor of Axillary Lymph Node Metastases in Breast Cancer
- Incidence of Axillary Lymph Node Metastases in T1 Breast Cancer
- Axillary Lymph Node Metastases in Patients with T1 Breast Carcinoma: Correlation with Histopathologic and Immunohistochemical Characteristics of the Primary Tumor
- Incidence of Axillary Lymph Node Metastases in T1 Breast Cancer
