A Case of Clonorchiasis with Focal Intrahepatic Duct Dilatation Mimicking an Intrahepatic Cholangiocarcinoma
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University College of Medicine, Yangsan, Korea. sulsulpul@yahoo.co.kr
Abstract
- Biliary strictures can be caused by various diseases. Intrahepatic duct (IHD) strictures are usually related to IHD stones and cholangitis. However, focal IHD strictures without IHD stones often create diagnostic problems. Parasitic diseases such as clonorchiasis can be a rare cause of an IHD stricture. Human clonorchiasis (Clonorchis sinensis infection) is an endemic parasitic disease in Eastern Asia, including Korea, and patients acquire the infestation by eating raw fish. On radiological examinations, clonorchiasis shows typically diffuse, minimal, or mild dilatation of the small IHD, particularly in the periphery, without dilatation of the extrahepatic duct. However, diagnosis of clonorchiasis can sometimes be difficult when radiological changes are atypical. We report a case of focal left IHD dilatation caused by clonorchiasis that was confused with a malignancy.
Keyword
MeSH Terms
Figure
-
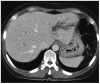
Fig. 1 Contrast-enhanced computed tomography scan finding. It shows the dilatation of left intrahepatic bile duct without mass or intrahepatic stone.

Fig. 2 Magnetic resonance cholangiopancreatography findings. (A) Axial T2 weighted image shows the marked dilatation and stricture (arrow) of left intrahepatic bile duct. (B) Coronal T2 weighted image shows the marked dilatation and stricture (arrow) of left intrahepatic bile duct. There is no evidence of stone and thickeness of duct wall at stricture segment.

Fig. 3 Cholangiographic findings. (A) Cholangioscope is inserted via a percutaneous transhepatic route. Radiograph shows the focal stricture (arrow) and dilatation of left intrahepatic duct (IHD) without abnormality of extrahepatic and right IHD. (B) After removal of the fluke, there is no evidence of filling defect at the left IHD.

Fig. 4 Percutaneous transhepatic cholangioscopy findings. (A) Dark brown, soft obstructive mass is found at stricture site of left intrahepatic duct. (B) Flat, leaf-shaped worm indentified as Clonorchis sinensis is observed after extraction of bile sludge. (C) The fluke is extracted with an endocopic forcep. After removal, there is no obvious stricture and surface irregularity or abnormal tumor vessel is not seen.
Reference
-
1. Seo DW, Kim MH, Lee SK, et al. Usefulness of cholangioscopy in patients with focal stricture of the intrahepatic duct unrelated to intrahepatic stones. Gastrointest Endosc. 1999; 49:204–209. PMID: 9925699.
Article2. Yeh YH, Huang MH, Yang JC, Mo LR, Lin J, Yueh SK. Percutaneous transhepatic cholangioscopy and lithotripsy in the treatment of intrahepatic stones: a study with 5 year follow-up. Gastrointest Endosc. 1995; 42:13–18. PMID: 7557170.
Article3. Kim TS, Cho SH, Huh S, et al. A nationwide survey on the prevalence of intestinal parasitic infections in the Republic of Korea, 2004. Korean J Parasitol. 2009; 47:37–47. PMID: 19290090.
Article4. Cho SH, Lee KY, Lee BC, et al. Prevalence of clonorchiasis in southern endemic areas of Korea in 2006. Korean J Parasitol. 2008; 46:133–137. PMID: 18830051.
Article5. Joo CY, Chung MS, Kim SJ, Kang CM. Changing patterns of Clonorchis sinensis infections in Kyongbuk, Korea. Korean J Parasitol. 1997; 35:155–164. PMID: 9335180.
Article6. Lee JI, Yoo JH, Lim GS, Lee CH, Min YI, Lim JH. ERCP findings in clonorchiasis. Korean J Gastrointest Endosc. 1981; 1:29–32.7. Kang DH, Choi SH, Chun KJ, et al. ERCP findings in hepatic clonorchiasis. Korean J Gastrointest Endosc. 1993; 13:121–125.8. Lim JH. Radiologic findings of clonorchiasis. AJR Am J Roentgenol. 1990; 155:1001–1008. PMID: 2120925.
Article9. Choi D, Hong ST. Imaging diagnosis of clonorchiasis. Korean J Parasitol. 2007; 45:77–85. PMID: 17570969.
Article10. Choi BI, Han JK, Hong ST, Lee KH. Clonorchiasis and cholangiocarcinoma: etiologic relationship and imaging diagnosis. Clin Microbiol Rev. 2004; 17:540–552. PMID: 15258092.
Article11. Song HY, Rhee KS, Lee ST, Kim DK, Ahn DS. Clinical features in clonorchiasis. Korean J Gastroenterol. 1995; 27:64–71.12. Chan HH, Lai KH, Lo GH, et al. The clinical and cholangiographic picture of hepatic clonorchiasis. J Clin Gastroenterol. 2002; 34:183–186. PMID: 11782616.
Article13. Jeen YM, Jin SY. Intrahepatic cholangiocarcinoma associated with Clonorchis sinensis infection. Korean J Hepatol. 2009; 15:524–527. PMID: 20037272.
Article14. Hwang CW, Lim BW, Ryu U, et al. A case of clonorchiasis presenting as common hepatic duct mass. Korean J Gastrointest Endosc. 2005; 31:268–272.15. Chu DW, Li JC, Lee DW, Rong ZX, Chen XW, Chan AC. Unusual presentations of hepatic clonorchiasis. Gastrointest Endosc. 2003; 58:637–639. PMID: 14520309.
Article16. Oh JH, Kim HG. A case of clonorchiasis presenting as common bile duct mass. Korean J Gastroenterol. 2010; 56:211–213. PMID: 20962555.
Article17. Yoon KW, Park CH, Cho S, et al. A case of hemobilia caused by clonorchiasis. Korean J Gastrointest Endosc. 2008; 36:313–317.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clonorchiasis and its complications: cholangiogram revisited
- Intrahepatic cholangiocarcinoma associated with Clonorchis sinensis infection
- Histopathology of a benign bile duct lesion in the liver: Morphologic mimicker or precursor of intrahepatic cholangiocarcinoma
- A Case of Clonorchiasis Presenting as Common Hepatic Duct Mass
- Mucin-Producing Intrahepatic Cholangiocelluar Carcinoma Presenting as a Focal Dilatation of the Intrahepatic Bile Duct
