Clinical, Radiologic, and Pathologic Findings of Subdural Osteoma: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, Inha University Hospital, Incheon, Korea. nsshim60@inha.ac.kr
- KMID: 2165234
- DOI: http://doi.org/10.14791/btrt.2016.4.1.40
Abstract
- We present a case of a subdural osteoma. A 29-year-old female presented with a 3-year history of headaches. Computed tomography scan revealed a homogeneous high-density lesion isolated from the inner table of the frontal bone (a lucent dural line) in the right frontal convexity. Magnetic resonance imaging revealed an extra-axial lesion with a broad base without dural tail sign and punctate enhancement pattern characteristic of abundant adipose tissue. Upon surgical excision, we found a hard bony mass clearly demarcated from the dura. The mass displayed characteristics of an osteoma upon histological examination. The symptom was relieved after operation.
Keyword
MeSH Terms
Figure
-
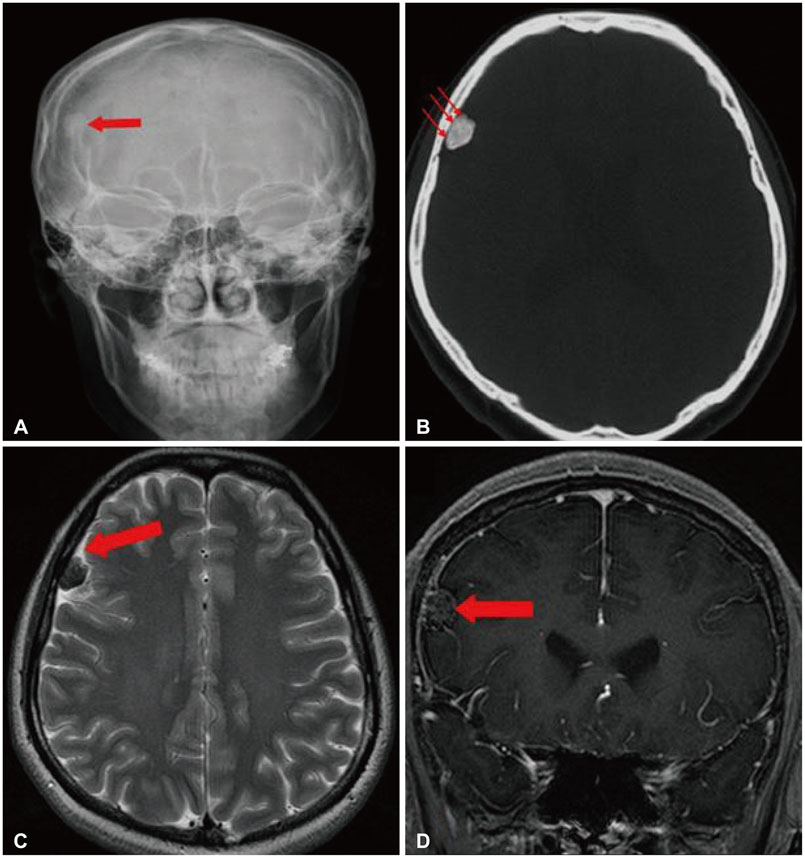
Fig. 1 A: Plain radiography showed a dense calcified mass in the right frontal area. B: CT scan of the bone window showed an intraparenchymal calcified lesion separated from bone. The arrows indicate a typical lucent dural line manifest in intracranial intraparenchymal osteoma. C: Magnetic resonance T2-weighted image. The arrow denotes cerebrospinal fluid under subarachnoid space. D: Gadolinium enhanced T1-weighted image showed the typical punctate enhancement pattern characteristic of abundant adipose tissue in osteoma. It is a consideration in differential diagnosis with meningioma.
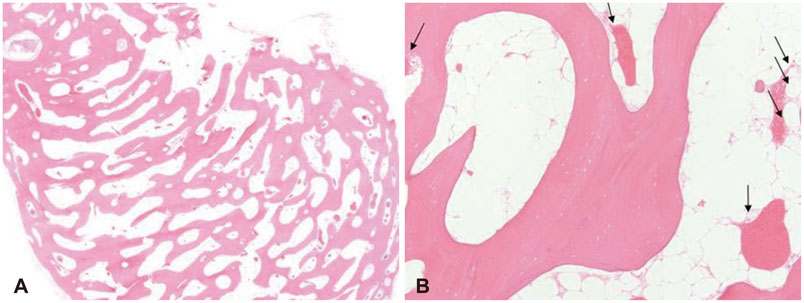
Fig. 2 Pathological findings. A: Microscopically lamellated bony trabeculae are lined by osteoblasts (H&E staining, ×10). B: The intertrabecular marrow spaces are occupied by abundant adipose cells and loose fibrovascular tissues (H&E staining, ×100). Endothelial cells (arrows) adhere to the osteoid layers. H&E, hematoxylin and eosin.
Reference
-
1. Cheon JE, Kim JE, Yang HJ. CT and pathologic findings of a case of subdural osteoma. Korean J Radiol. 2002; 3:211–213.
Article2. Kim JK, Lee KJ, Cho JK, et al. Intracranial intraparenchymal ostemoa. J Korean Neurosurg Soc. 1998; 27:1450–1454.3. Jung TY, Jung S, Jin SG, Jin YH, Kim IY, Kang SS. Solitary intracranial subdural osteoma: intraoperative findings and primary anastomosis of an involved cortical vein. J Clin Neurosci. 2007; 14:468–470.
Article4. Lee ST, Lui TN. Intracerebral osteoma: case report. Br J Neurosurg. 1997; 11:250–252.
Article5. Vakaet A, De Reuck J, Thiery E, vander Eecken H. Intracerebral osteoma: a clinicopathologic and neuropsychologic case study. Childs Brain. 1983; 10:281–285.
Article6. Haddad FS, Haddad GF, Zaatari G. Cranial osteomas: their classification and management. Report on a giant osteoma and review of the literature. Surg Neurol. 1997; 48:143–147.
Article7. Akiyama M, Tanaka T, Hasegawa Y, Chiba S, Abe T. Multiple intracranial subarachnoid osteomas. Acta Neurochir (Wien). 2005; 147:1085–1089. discussion 1089.
Article8. Pau A, Chiaramonte G, Ghio G, Pisani R. Solitary intracranial subdural osteoma: case report and review of the literature. Tumori. 2003; 89:96–98.
Article9. Aoki H, Nakase H, Sakaki T. Subdural osteoma. Acta Neurochir (Wien). 1998; 140:727–728.
Article10. Choudhury AR, Haleem A, Tjan GT. Solitary intradural intracranial osteoma. Br J Neurosurg. 1995; 9:557–559.
Article11. Constantinidis J. [Intrathalamic osteoma]. Psychiatr Neurol (Basel). 1967; 154:366–372.
