Acute Paraplegia as a Result of Hemorrhagic Spinal Ependymoma Masked by Spinal Anesthesia: Case Report and Review of Literature
- Affiliations
-
- 1Department of Neurosurgery, Seoul St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea. jhyun@catholic.ac.kr
- KMID: 2165232
- DOI: http://doi.org/10.14791/btrt.2016.4.1.30
Abstract
- Ependymomas are the most common intramedullary spinal cord tumors in adults. Although a hemorrhage within spinal ependymoma on imaging studies is not uncommon, it has rarely been reported to bea cause of acute neurological deficit. In the present report, we describe a case of a 24-year-old female patient who developed acute paraplegia as a result of hemorrhagic spinal ependymoma immediately after a cesarean delivery under spinal regional anesthesia. We review the literature of hemorrhagic spinal ependymomas presenting with acute neurological deficit and discuss the most appropriate treatment for a good neurological recovery.
Keyword
MeSH Terms
Figure
-

Fig. 1 Initial spinal magnetic resonance image (MRI) scan. A: T2-weighted MRI shows an abnormal spinal cord lesion from C2 level to D5. A spinal cord swelling with an irregular high signal intensity is noted in T2-weighted image. The margin is poorly demarcated. Most part of the lesion is suspicious of a syrinx formation or a hemorrhage. B: The lesion shows the low signal intensity in T1-weighted MRI. C: Gadolinium-enhanced T1-weighted MRI shows a heterogeneously enhancing lesion from C6 to D2. There is no abnormal intradural lesion in the proximal and distal areas.
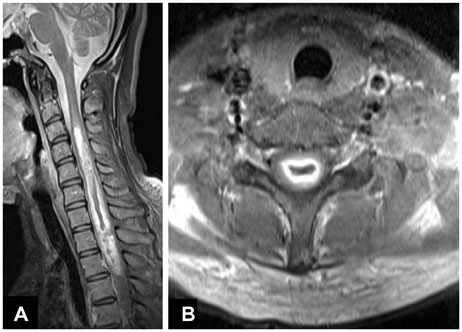
Fig. 2 Preoperative spinal MRI scan after 2 weeks of medical treatment. A: Preoperative gadolinium-enhanced T1-weighted MRI shows a heterogeneously enhancing mass from C3 level to D2 level. B: Axial cut of gadolinium-enhanced T1-weighted MRI shows a dark central portion with the margin enhancement.
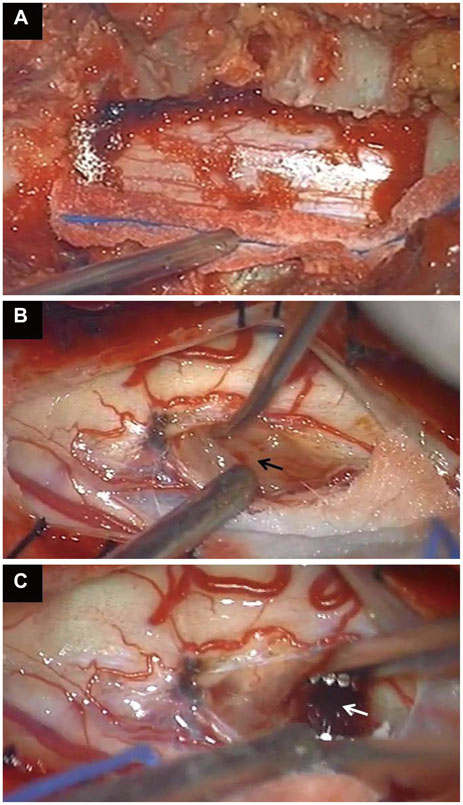
Fig. 3 Intraoperative findings. A: Unilateral hemilaminectomies were performed on the left side of C7 and T1 level. B: After opening the dura, a midline incision was done precisely at the spinal cord. A gray and sticky mass was observed below the midline pial incision (arrow). C: After removing the mass partially, a dark hematoma was observed inside the mass (arrow) and a large amount of the dark hematoma could be sucked out easily.
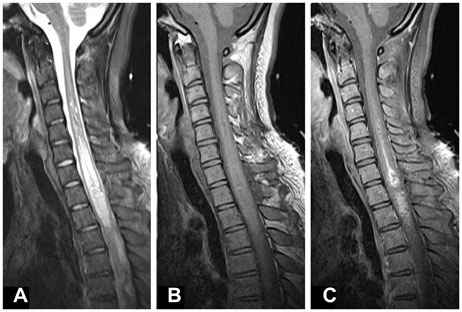
Fig. 4 Postoperative spinal MRI scan. A huge amount of the abnormal lesion decreased. A: T2-weighted MRI shows a hyper-intense lesion from C4 level to D2 level. B: T1-weighted MRI shows the same lesion in the low signal intensity. C: Enhancing portion is much more decreased in gadolinium-enhanced T1-weighted MRI as compared to the preoperative MRI scan. The remaining lesion is mainly from C7 to D2 level.

Fig. 5 Spinal MRI scan taken 1 week after the first surgery (preoperative MRI for the second surgery). A: Gadolinium-enhanced T1-weighted MRI shows that the enhancing mass diminished significantly and was partially removed at T1 level. B: Axial image of gadolinium-enhanced T1-weighted MRI shows a dark central portion which was the hematoma totally removed and the nhancing portion remained.

Fig. 6 Postoperative spinal MRI scan after the second surgery. A: Gadolinium-enhanced T1-weighted MRI shows that most of the enhancing portion was removed and only a very thin-layered enhancing portion remained. B: Axial image of gadolinium-enhanced T1-weighted MRI shows a thin-layered enhancing portion remaining at C7 level.
Reference
-
1. Martinez-Perez R, Hernandez-Lain A, Paredes I, Munarriz PM, Castaño-Leon AM, Lagares A. Acute neurological deterioration as a result of two synchronous hemorrhagic spinal ependymomas. Surg Neurol Int. 2012; 3:33.
Article2. Rawlings CE 3rd, Giangaspero F, Burger PC, Bullard DE. Ependymomas: a clinicopathologic study. Surg Neurol. 1988; 29:271–281.
Article3. Schweitzer JS, Batzdorf U. Ependymoma of the cauda equina region: diagnosis, treatment, and outcome in 15 patients. Neurosurgery. 1992; 30:202–207.4. Yoshii S, Shimizu K, Ido K, Nakamura T. Ependymoma of the spinal cord and the cauda equina region. J Spinal Disord. 1999; 12:157–161.
Article5. Admiraal P, Hazenberg GJ, Algra PR, Kamphorst W, Wolbers JG. Spinal subarachnoid hemorrhage due to a filum terminale ependymoma. Clin Neurol Neurosurg. 1992; 94:69–72.
Article6. Destée A, Lesoin F, Warot M, Mendolia G, Devos P, Warot P. [Tumoral spinal meningeal hemorrhage during anticoagulant treatment]. Rev Neurol (Paris). 1984; 140:517–519.7. Herb E, Schwachenwald R, Nowak G, Müller H, Reusche E. Acute bleeding into a filum terminale ependymoma. Neurosurg Rev. 1990; 13:243–245.
Article8. Heuer GG, Stiefel MF, Bailey RL, Schuster JM. Acute paraparesis from hemorrhagic spinal ependymoma: diagnostic dilemma and surgical management. Report of two cases and review of the literature. J Neurosurg Spine. 2007; 7:652–655.
Article9. Malbrain ML, Kamper AM, Lambrecht GL, et al. Filum terminale ependymoma revealed by acute cauda equina compression syndrome following intratumoral and spinal subarachnoid hemorrhage in a patient on oral anticoagulants. Acta Neurol Belg. 1994; 94:35–43.10. Oertel J, Gaab MR, Piek J. Partial recovery of paraplegia due to spontaneous intramedullary ependyma haemorrhage. Acta Neurochir (Wien). 2000; 142:219–220.
Article11. Rivierez M, Oueslati S, Philippon J, et al. [Ependymoma of the intradural filum terminale in adults. 20 cases]. Neurochirurgie. 1990; 36:96–107.12. Tait MJ, Chelvarajah R, Garvan N, Bavetta S. Spontaneous hemorrhage of a spinal ependymoma: a rare cause of acute cauda equina syndrome: a case report. Spine (Phila Pa 1976). 2004; 29:E502–E505.13. Lagares A, Rivas JJ, Lobato RD, Ramos A, Alday R, Boto GR. Spinal cord ependymoma presenting with acute paraplegia due to tumoral bleeding. J Neurosurg Sci. 2000; 44:95–97. discussion 97-8.14. Klekamp J. Spinal ependymomas. Part 1: Intramedullary ependymomas. Neurosurg Focus. 2015; 39:E6.
Article15. Kucia EJ, Bambakidis NC, Chang SW, Spetzler RF. Surgical technique and outcomes in the treatment of spinal cord ependymomas, part 1: intramedullary ependymomas. Neurosurgery. 2011; 68:1 Suppl Operative. 57–63. discussion 63.
Article16. Lee SH, Chung CK, Kim CH, et al. Long-term outcomes of surgical resection with or without adjuvant radiation therapy for treatment of spinal ependymoma: a retrospective multicenter study by the Korea Spinal Oncology Research Group. Neuro Oncol. 2013; 15:921–929.
Article17. Oh MC, Ivan ME, Sun MZ, et al. Adjuvant radiotherapy delays recurrence following subtotal resection of spinal cord ependymomas. Neuro Oncol. 2013; 15:208–215.
Article18. Safaee M, Oh MC, Mummaneni PV, et al. Surgical outcomes in spinal cord ependymomas and the importance of extent of resection in children and young adults. J Neurosurg Pediatr. 2014; 13:393–399.
Article19. Gavin Quigley D, Farooqi N, Pigott TJ, et al. Outcome predictors in the management of spinal cord ependymoma. Eur Spine J. 2007; 16:399–404.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Paraplegia due to Spinal Epidermoid Cyst Rupture at Asthma Attack
- Neurologic Complication Following Spinal Epidural Anesthesia in a Patient with Spinal Intradural Extramedullary Tumor
- Paraplegia due to Spinal Cord Infarction After Lifting Heavy Objects
- A Case of Intramedullary Ependymoma in the upper Thoracic Spinal Cord
- Paraplegia Due to Spinal Hematoma in a Patient with Acute Lymphocytic Leukemia: A case report
