Inflamed Symptomatic Sellar Arachnoid Cyst: Case Report
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University, Seoul, Korea.
- 2Neurooncology Clinic, National Cancer Center of Korea, Goyang, Korea. nsghs@ncc.re.kr
- 3Department of Pathology, National Cancer Center of Korea, Goyang, Korea.
- 4Department of Radiology, National Cancer Center of Korea, Goyang, Korea.
- KMID: 2165219
- DOI: http://doi.org/10.14791/btrt.2013.1.1.28
Abstract
- Sellar arachnoid cysts are rare; an infected arachnoid cyst is extremely rare as only one case has been reported to date in the literature. Here, we report a patient with an infected or inflamed sellar arachnoid cyst that was successfully treated with transsphenoidal surgery (TSA). A 53-year-old female with a history of chronic sinusitis developed a headache 5 months ago, and one month before admission polyuria, polydipsia, and abnormal vaginal bleeding occurred. The magnetic resonance imaging (MRI) showed a sellar cystic mass with a thickened pituitary stalk. Preoperative hormonal study revealed normal pituitary hormone levels except for a moderate elevation of prolactin. She was diagnosed with diabetes insipidus of the central nervous system origin based on a water-deprivation test. TSA was performed under an impression of symptomatic Rathke's cleft cyst according to the MRI findings. Intraoperative findings showed confirmation of turbid intracystic contents, but micro-organisms were unidentified on microbial culture. Pathology of the cyst wall revealed inflamed meningoepithelial lining cells compatible with an arachnoid cyst.
Keyword
MeSH Terms
Figure
-

Fig. 1 Preoperative MR images. Axial T1 non-enhanced (A) and gadolinium enhanced (B) images show a well-defined intrasellar cystic lesion, and the wall is faintly enhanced. FLAIR image suggested the content of cyst was not CSF but high proteinous material, which was compatible with Rathke's cleft cyst (C). Enhanced sagittal image showed that the cyst was attached to the thickened pituitary stalk and displaced the pituitary gland inferiorly (D). MR: magnetic resonance, CSF: cerebrospinal fluid, FLAIR: fluid attenuated inversion recovery.
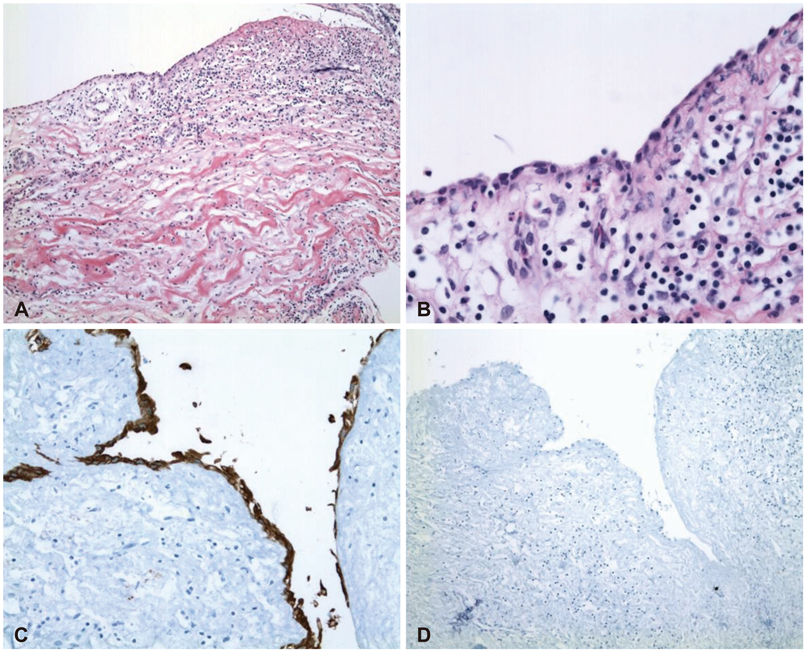
Fig. 2 Photomicrograph of the cyst. The inner layer of the cyst wall shows a single layer of flattened meningothelial cells and the outer layer is composed of collagenous tissue, slightly thickened by mononuclear inflammatory cell infiltration and edema (hematoxilin and eosin; A: ×100, B: ×200). The immunohistochemical stains of the lining cells of the cyst are positive for epithelial membrane antigen (C) and negative for glial fibrillar acidic protein (D), which is consistent with an arachnoid cyst. There is no glial tissue in the outer layer of the cyst (×200).
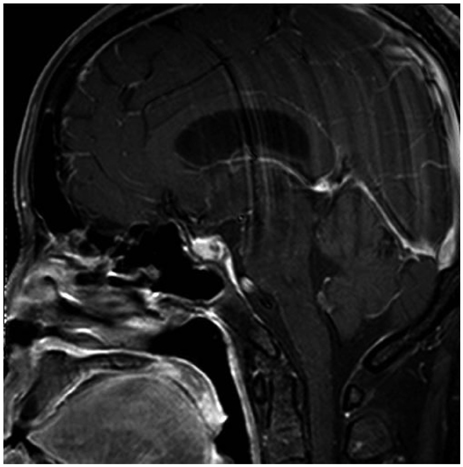
Fig. 3 MRI taken 3 months postoperatively showing disappearance of previous sellar cyst and preserved pituitary gland and stalk. MRI: magnetic resonance imaging.
Reference
-
1. Eskandary H, Sabba M, Khajehpour F, Eskandari M. Incidental findings in brain computed tomography scans of 3000 head trauma patients. Surg Neurol. 2005; 63:550–553. discussion 553.
Article2. Katzman GL, Dagher AP, Patronas NJ. Incidental findings on brain magnetic resonance imaging from 1000 asymptomatic volunteers. JAMA. 1999; 282:36–39.
Article3. Weber F, Knopf H. Incidental findings in magnetic resonance imaging of the brains of healthy young men. J Neurol Sci. 2006; 240:81–84.
Article4. Rengachary SS, Watanabe I. Ultrastructure and pathogenesis of intracranial arachnoid cysts. J Neuropathol Exp Neurol. 1981; 40:61–83.
Article5. Dubuisson AS, Stevenaert A, Martin DH, Flandroy PP. Intrasellar arachnoid cysts. Neurosurgery. 2007; 61:505–513. discussion 513.
Article6. Miyajima M, Arai H, Okuda O, Hishii M, Nakanishi H, Sato K. Possible origin of suprasellar arachnoid cysts: neuroimaging and neurosurgical observations in nine cases. J Neurosurg. 2000; 93:62–67.
Article7. Rohrer DC, Burchiel KJ, Gruber DP. Intraspinal extradural meningeal cyst demonstrating ball-valve mechanism of formation. Case report. J Neurosurg. 1993; 78:122–125.
Article8. Sivaraman V, Au-Yeung A, Brew S, McEvoy AW, Greenwood R. An infected arachnoid cyst in an elderly patient. J Neurol. 2008; 255:1088–1089.
Article9. Shin JL, Asa SL, Woodhouse LJ, Smyth HS, Ezzat S. Cystic lesions of the pituitary: clinicopathological features distinguishing craniopharyngioma, Rathke's cleft cyst, and arachnoid cyst. J Clin Endocrinol Metab. 1999; 84:3972–3982.
Article10. Miyamoto T, Ebisudani D, Kitamura K, Ohshima T, Horiguchi H, Nagahiro S. Surgical management of symptomatic intrasellar arachnoid cysts--two case reports. Neurol Med Chir (Tokyo). 1999; 39:941–945.
Article
