Clin Endosc.
2016 Mar;49(2):202-206. 10.5946/ce.2015.059.
Tracheal Involvement in Crohn Disease: the First Case in Korea
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. H00095@paik.ac.kr
- 2Division of Pulmonology, Department of Internal Medicine, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
- 3Department of Pathology, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2165047
- DOI: http://doi.org/10.5946/ce.2015.059
Abstract
- Respiratory involvement in Crohn disease (CD) is rare condition with only about a dozen reported cases. We report the first case of CD with tracheal involvement in Korea. An 18-year-old woman with CD was hospitalized because of coughing, dyspnea, and fever sustained for 3 weeks. Because she had stridor in her neck, we performed computed tomography of the neck, which showed circumferential wall thickening of the larynx and hypopharynx. Bronchoscopy revealed mucosal irregularity, ulceration, and exudates debris in the proximal trachea, and bronchial biopsy revealed chronic inflammation with granulation tissue. Based on these findings, we suspected CD with tracheal involvement and began administering intravenous methylprednisolone at 1 mg/kg per day, after which her symptoms and bronchoscopic findings improved.
MeSH Terms
Figure
-
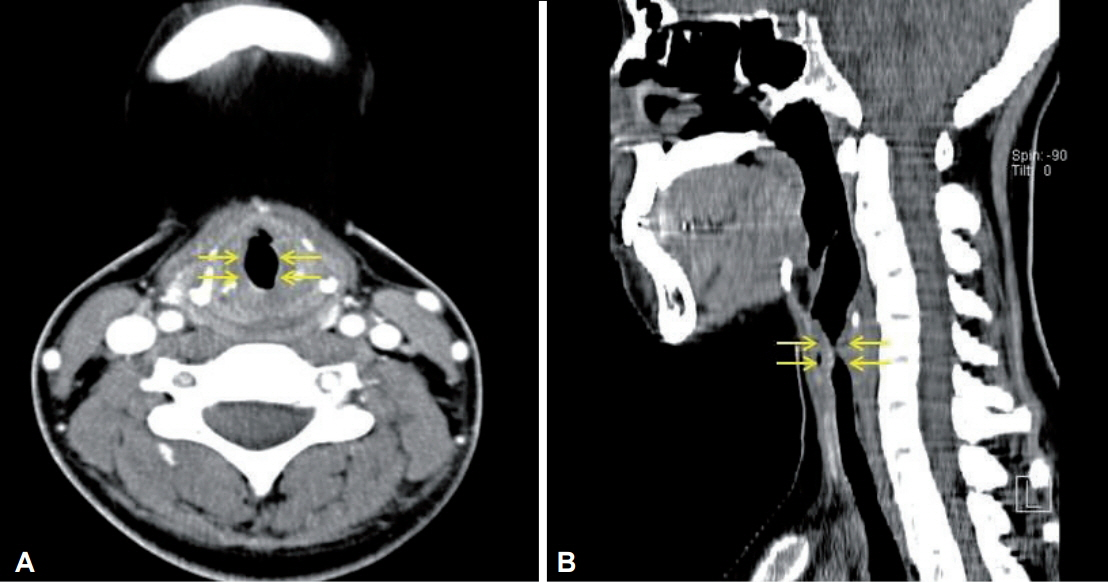
Fig. 1. (A, B) Computed tomography of neck showed abrupt narrowing of proximal trachea (arrows).

Fig. 2. Flexible bronchoscopy showed mucosal irregularity, edema, and yellowish patch-like mucosal lesion on the proximal part of trachea.

Fig. 3. Bronchoscopic biopsy. (A) Dense inflammatory cell infiltration in the mucosa and submucosa of trachea (H&E stain, ×10). (B) Granulation tissue representing healing of damaged tissue (H&E stain, ×100).

Fig. 4. Flexible bronchoscopy findings after treatment show marked improvement.
Reference
-
1. Spira A, Grossman R, Balter M. Large airway disease associated with inflammatory bowel disease. Chest. 1998; 113:1723–1726.
Article2. Henry MT, Davidson LA, Cooke NJ. Tracheobronchial involvement with Crohn’s disease. Eur J Gastroenterol Hepatol. 2001; 13:1495–1497.
Article3. Asami T, Koyama S, Watanabe Y, et al. Tracheobronchitis in a patient with Crohn’s disease. Intern Med. 2009; 48:1475–1478.
Article4. Camus P, Colby TV. The lung in inflammatory bowel disease. Eur Respir J. 2000; 15:5–10.
Article5. Kraft SC, Earle RH, Roesler M, Esterly JR. Unexplained bronchopulmonary disease with inflammatory bowel disease. Arch Intern Med. 1976; 136:454–459.
Article6. Kuźniar T, Sleiman C, Brugière O, et al. Severe tracheobronchial stenosis in a patient with Crohn’s disease. Eur Respir J. 2000; 15:209–212.
Article7. Ulrich R, Goldberg R, Line WS. Crohn’s disease: a rare cause of upper airway obstruction. J Emerg Med. 2000; 19:331–332.
Article8. Lemann M, Messing B, D’Agay F, Modigliani R. Crohn’s disease with respiratory tract involvement. Gut. 1987; 28:1669–1672.
Article9. Iwama T, Higuchi T, Imajo M, Akagawa S, Matsubara O, Mishima Y. Tracheo-bronchitis as a complication of Crohn’s disease: a case report. Jpn J Surg. 1991; 21:454–457.
Article10. Hotermans G, Benard A, Guenanen H, Demarcq-Delerue G, Malart T, Wallaert B. Nongranulomatous interstitial lung disease in Crohn’s disease. Eur Respir J. 1996; 9:380–382.
Article11. Plataki M, Tzortzaki E, Lambiri I, Giannikaki E, Ernst A, Siafakas NM. Severe airway stenosis associated with Crohn’s disease: case report. BMC Pulm Med. 2006; 6:7.
Article12. Kelly JH, Montgomery WW, Goodman ML, Mulvaney TJ. Upper airway obstruction associated with regional enteritis. Ann Otol Rhinol Laryngol. 1979; 88(1 Pt 1):95–99.
Article13. Lamblin C, Copin MC, Billaut C, et al. Acute respiratory failure due to tracheobronchial involvement in Crohn’s disease. Eur Respir J. 1996; 9:2176–2178.
Article14. Kinebuchi S, Oohashi K, Takada T, et al. Tracheo-bronchitis associated with Crohn’s disease improved on inhaled corticotherapy. Intern Med. 2004; 43:829–834.
Article15. Ahmed KA, Thompson JW, Joyner RE, Stocks RM. Airway obstruction secondary to tracheobronchial involvement of asymptomatic undiagnosed Crohn’s disease in a pediatric patient. Int J Pediatr Otorhinolaryngol. 2005; 69:1003–1005.
Article16. Casey MB, Tazelaar HD, Myers JL, et al. Noninfectious lung pathology in patients with Crohn’s disease. Am J Surg Pathol. 2003; 27:213–219.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Duodenal Crohn's Disease: A case report
- Crohn's Disease with Oral and Tonsillar Ulceration
- Isolated Crohn's Disease of Stomach A case report and review of the literature
- Primary hypertrophic osteoarthropathy accompanied by Crohn's disease: a case report
- Crohn's Disease Initially Presenting as Vulvar Swelling
