Delayed Severe Hemobilia after Endoscopic Biliary Plastic Stent Insertion
- Affiliations
-
- 1Department of Internal Medicine, SAM Anyang Hospital, Anyang, Korea. permi@naver.com
- KMID: 2165027
- DOI: http://doi.org/10.5946/ce.2015.081
Abstract
- Hemobilia is a rare gastrointestinal bleeding, usually caused by injury to the bile duct. Hemobilia after endoscopic retrograde cholangiopancreatography (ERCP) is generally self-limiting and patients will spontaneously recover, but some severe and fatal hemorrhages have been reported. ERCP-related bowel or bile duct perforation should be managed promptly, according to the type of injury and the status of the patient. We recently experienced a case of late-onset severe hemobilia in which the patient recovered after endoscopic biliary stent insertion. The problem was attributable to ERCP-related bile duct perforation during stone removal, approximately 5 weeks prior to the hemorrhagic episode. The removal of the stent was performed 10 days before the onset of hemobilia. The bleeding was successfully treated by two sessions of transarterial coil embolization.
MeSH Terms
Figure
-
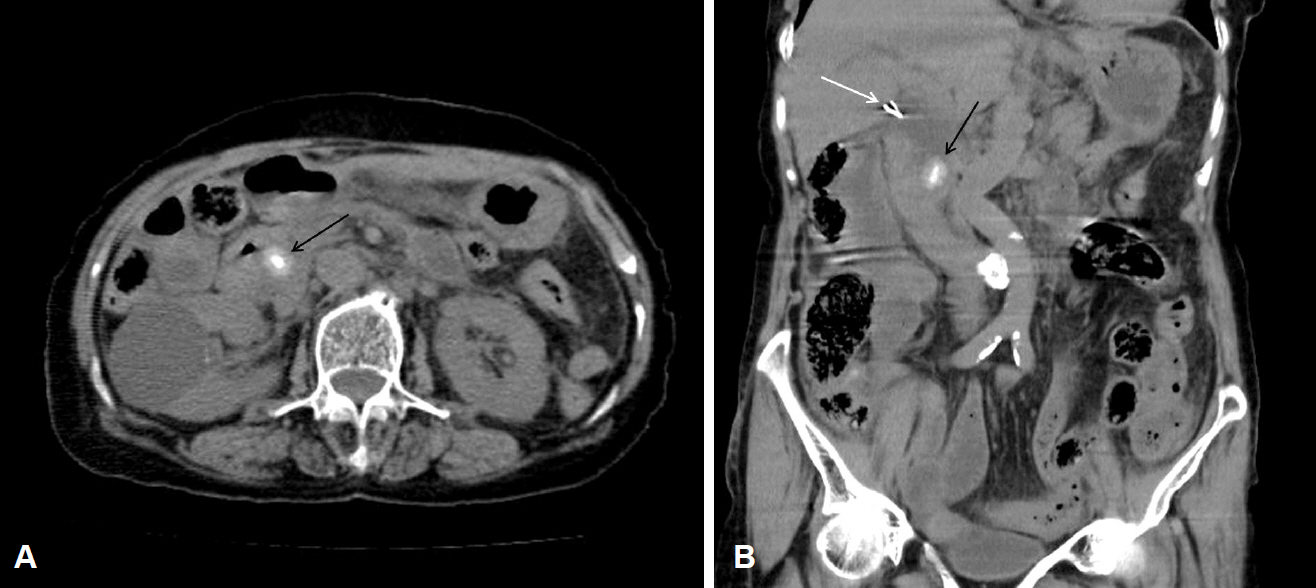
Fig. 1. (A, B) Abdominal non-enhanced computed tomography shows 15 mm-sized calcified stone in common bile duct (black arrow) and surgical clips are seen at the level of common haptic duct (white arrow).
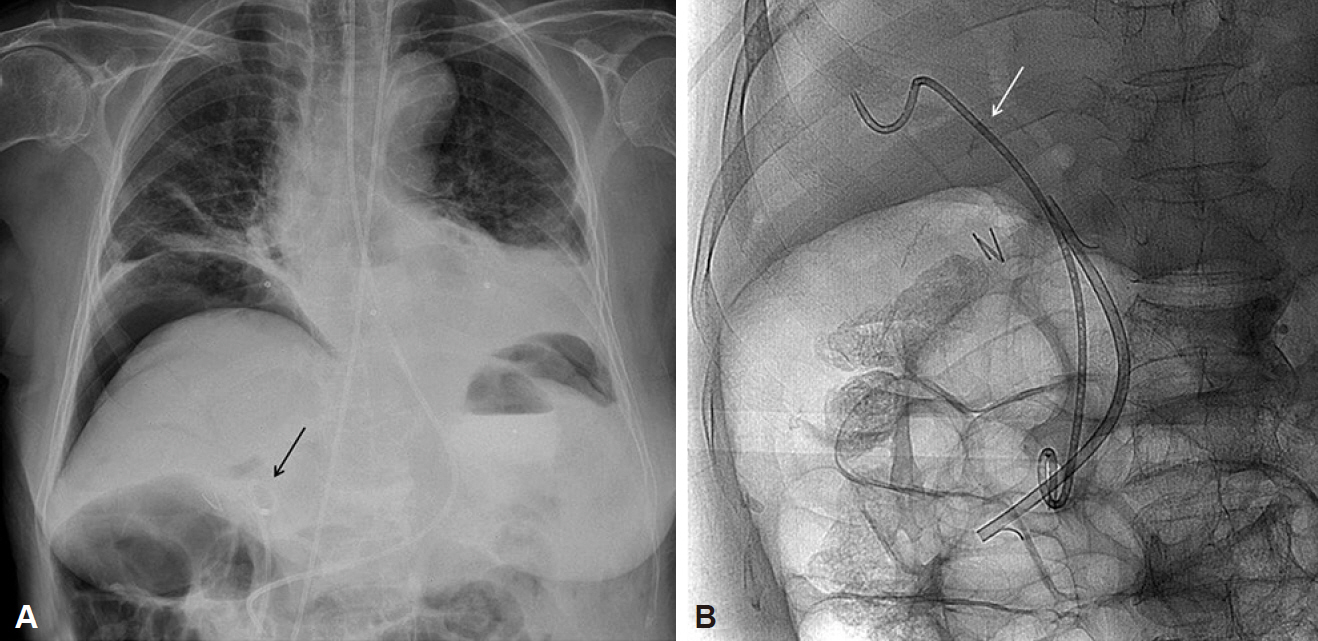
Fig. 2. Post-endoscopic retrograde cholangiopancreatography. (A) Chest radiography shows a large pneumoperitoneum under the right hemidiaphragm and nasobiliary drainage tube is also seen in the common bile duct is (black arrow) with air-biliarygram in the right anterior hepatic duct. (B) Two plastic biliary stents (one pigtail type [white arrow], the other straight type) are deeply located into the right hepatic duct.
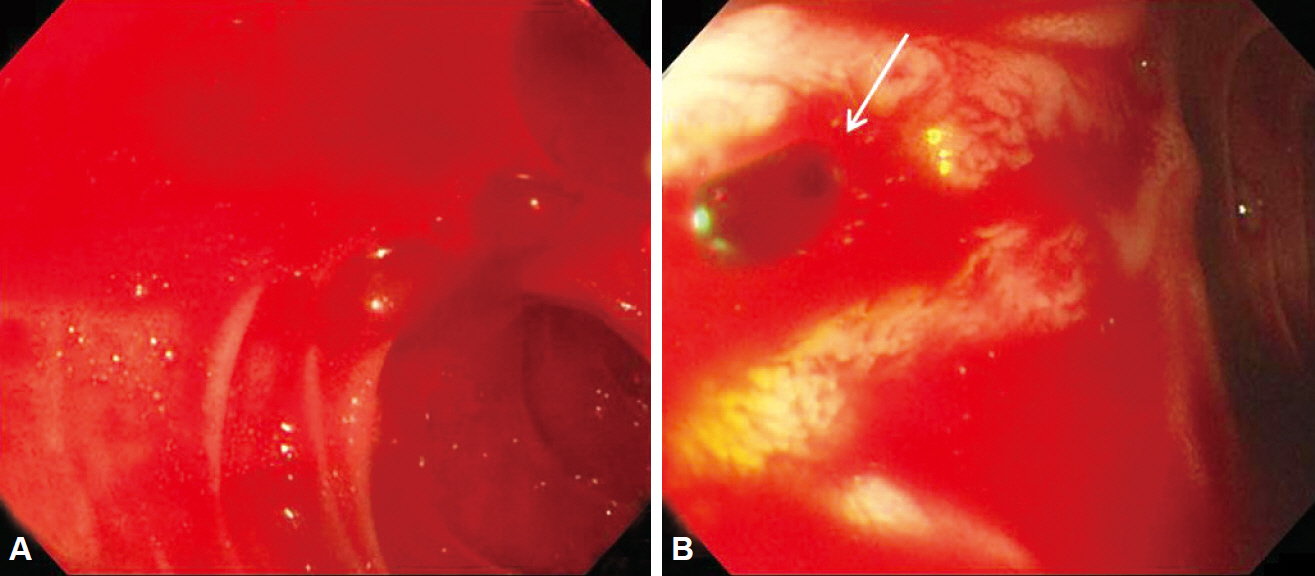
Fig. 3. (A, B) Emergent upper gastrointestinal endoscopy shows profuse active bleeding in the duodenum and the identified source of bleeding was the papillary orifice (white arrow), which is consistent with hemobilia.
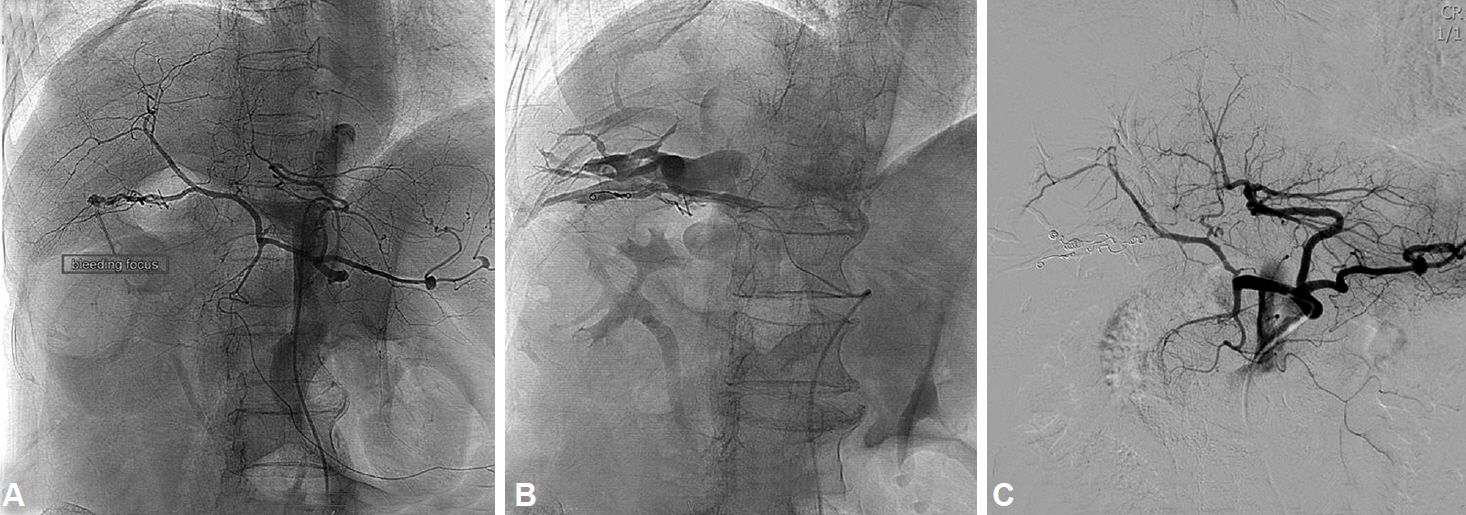
Fig. 4. Transarterial angiogram via celiac artery. (A) The left panel shows the extravasation of contrast material in the right posterior hepatic artery (RPHA), which is suggestive for active bleeding. (B) Cholangiogram of the right posterior hepatic duct is obtained through the arteriobiliary fistula near the RPHA. (C) After two sessions of embolization by using multiple coils, no further contrast extravasation is seen in right panel.
Reference
-
1. Goffette PP, Laterre PF. Traumatic injuries: imaging and intervention in post-traumatic complications (delayed intervention). Eur Radiol. 2002; 12:994–1021.
Article2. Lee SM, Cho KB. Value of temporary stents for the management of perivaterian perforation during endoscopic retrograde cholangiopancreatography. World J Clin Cases. 2014; 2:689–697.
Article3. Nezu Y, Nakaji S, Fujii H, Ishii E, Hirata N. Pseudoaneurysm caused by a self-expandable metal stent: a report of three cases. Endoscopy. 2014; 46:248–251.
Article4. Jeong HS, Shin TB, Hwang JC, Bae JI, Kim CW. Interventional management of delayed and massive hemobilia due to arterial erosion by metallic biliary stent. J Korean Soc Radiol. 2012; 66:27–33.
Article5. Rai R, Rose J, Manas D. Potentially fatal haemobilia due to inappropriate use of an expanding biliary stent. World J Gastroenterol. 2003; 9:2377–2378.
Article6. Watanabe M, Shiozawa K, Mimura T, et al. Hepatic artery pseudoaneurysm after endoscopic biliary stenting for bile duct cancer. World J Radiol. 2012; 4:115–120.
Article7. Layec S, D’Halluin PN, Pagenault M, Bretagne JF. Massive hemobilia during extraction of a covered self-expandable metal stent in a patient with portal hypertensive biliopathy. Gastrointest Endosc. 2009; 70:555–556.
Article8. Conio M, Caroli-Bosc FX, Buckley M, Chiaramondia M, D’Addazio G, Munizzi F. Massive hematobilia after extraction of plastic biliary endoprosthesis. J Clin Gastroenterol. 1997; 25:706.
Article9. Park JY, Ryu H, Bang S, Song SY, Chung JB. Hepatic artery pseudoaneurysm associated with plastic biliary stent. Yonsei Med J. 2007; 48:546–548.
Article10. Wolters F, Ryan B, Beets-Tan R, Dejong C. Delayed massive hemobilia after biliary stenting. Endoscopy. 2003; 35:976–977.
Article11. Bloechle C, Izbicki JR, Rashed MY, et al. Hemobilia: presentation, diagnosis, and management. Am J Gastroenterol. 1994; 89:1537–1540.12. Kim KH, Kim TN. Etiology, clinical features, and endoscopic management of hemobilia: a retrospective analysis of 37 cases. Korean J Gastroenterol. 2012; 59:296–302.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Delayed Hemobilia Caused by Penetration of Biliary Plastic Stent into Portal Vein
- Pancreaticoduodenal artery pseudoaneurysm-induced hemobilia caused by a plastic biliary stent
- Life-threatening Hemobilia following Removal of a Biliary Stent in a Patient with a Bile Leak
- Portal cavernography during endoscopic retrograde cholangiopancreatography: from bilhemia to hemobilia
- Percutaneous Endoscopic Biliary Stenting
