Multiple Rectal Neuroendocrine Tumors: Report of Five Cases
- Affiliations
-
- 1Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea. dr9696@nate.com
- KMID: 2164421
- DOI: http://doi.org/10.4166/kjg.2014.64.2.103
Abstract
- Carcinoids are slow growing neuroendocrine tumors (NET) originating in the enterochromaffin cells of the gastrointestinal tract. In previous studies, rectal NET comprised only about 1% of all anorectal neoplasms; however, the incidence of rectal NET has shown a recent increase. Typically, rectal NET presents as a single subepithelial nodule, and multicentricity of rectal NETs is rare, with reported incidence of 2-4.5%. Due to the rarity of multiple rectal NETs, there is no consensus or guidelines for treatment of multiple rectal NETs. However, NETs of the rectum that are less than 10 mm in diameter and do not infiltrate the muscularis propria, without distant metastasis, can be removed by endoscopy, as with solitary rectal NET. We encountered five cases of multiple rectal NETs which were treated successfully by endoscopy.
Keyword
MeSH Terms
Figure
-
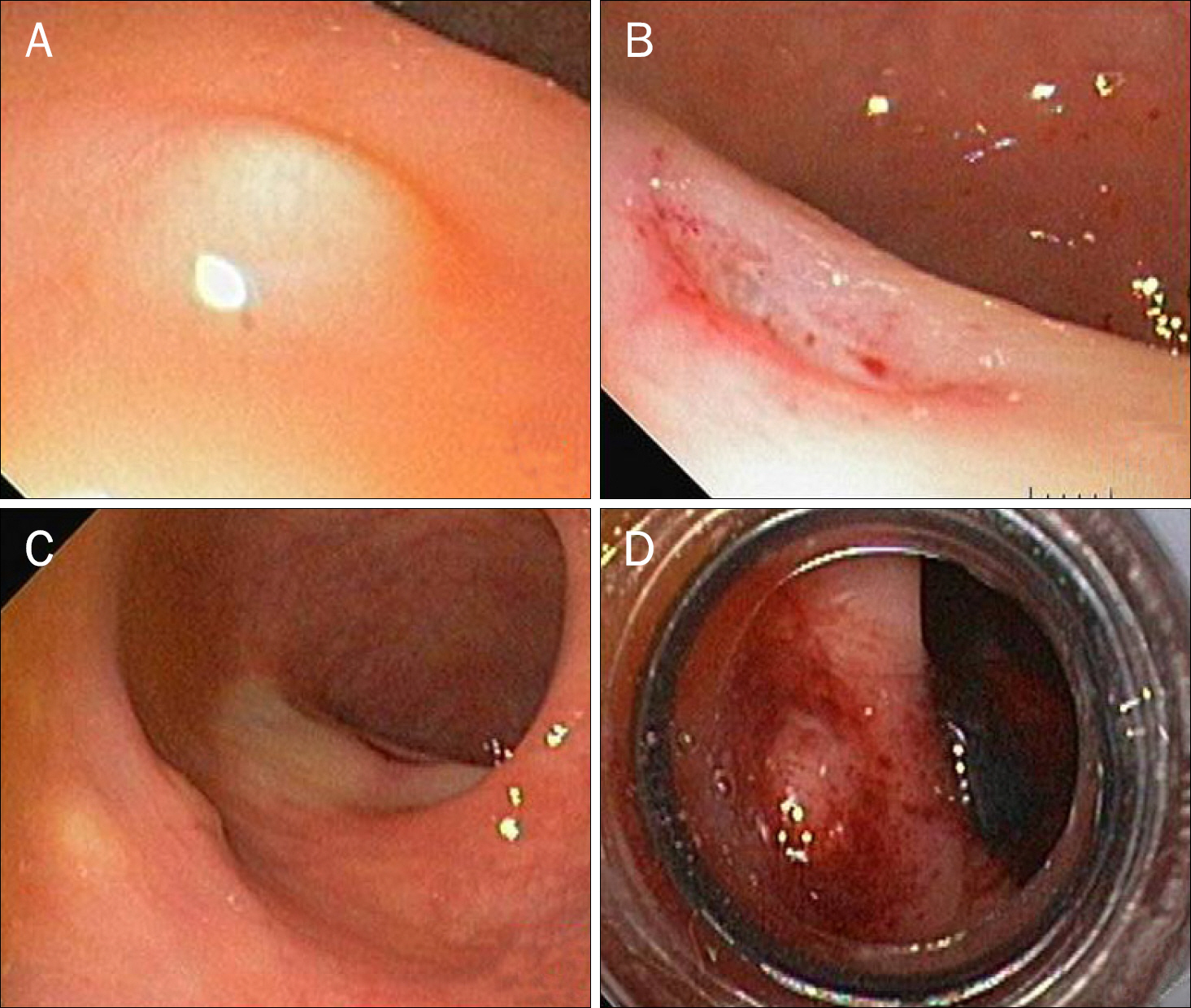
Fig. 1. Endoscopic views. (A) A small subepithelial nodule at the rectum was observed. (B) The small nodule was removed by biopsy. (C) Two other subepithelial nodules distal to the lesion (A) were observed. (D) Two subepithelial nodules were removed by endoscopic submucosal resection using a ligation device.
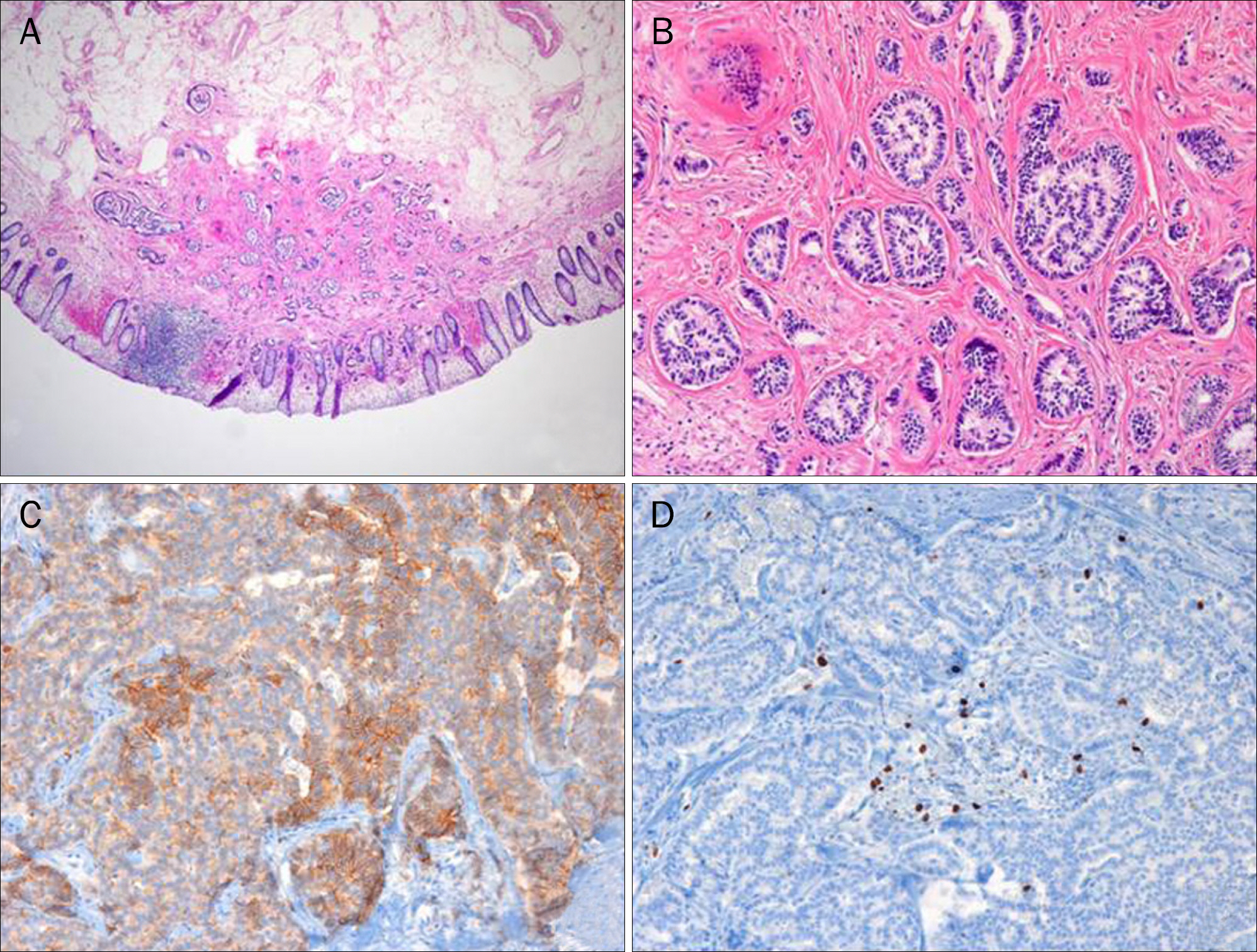
Fig. 2. Pathologic findings. (A) Carcinoid tumor is arising from lamina propria and infiltrating to the upper portion of submucosa (H&E, ×40).(B) Tumor cells forming a mostly glandular and trabecular pattern (H&E, ×100). (C) CD56 immunohistochemical staining is positive along the tumor cell membrane (×200). (D) Few Ki-67 nuclear stain positive cells are observed in the tumor (×200).

Fig. 3. Endoscopic submucosal resection using a ligation device (ESMR-L) technique. (A) Yellowish triple subepithelial lesions at the rectum were noted. (B) Lifting of lesions by hypertonic saline injection and band ligation are noted. (C) Triple rectal carcinoids were removed by ESMR-L.

Fig. 4. Endoscopic views. (A) Bleeding related to the endoscopic submucosal resection using a ligation device was noted. (B) Bleeding was controlled by endoscopic hemoclipping.
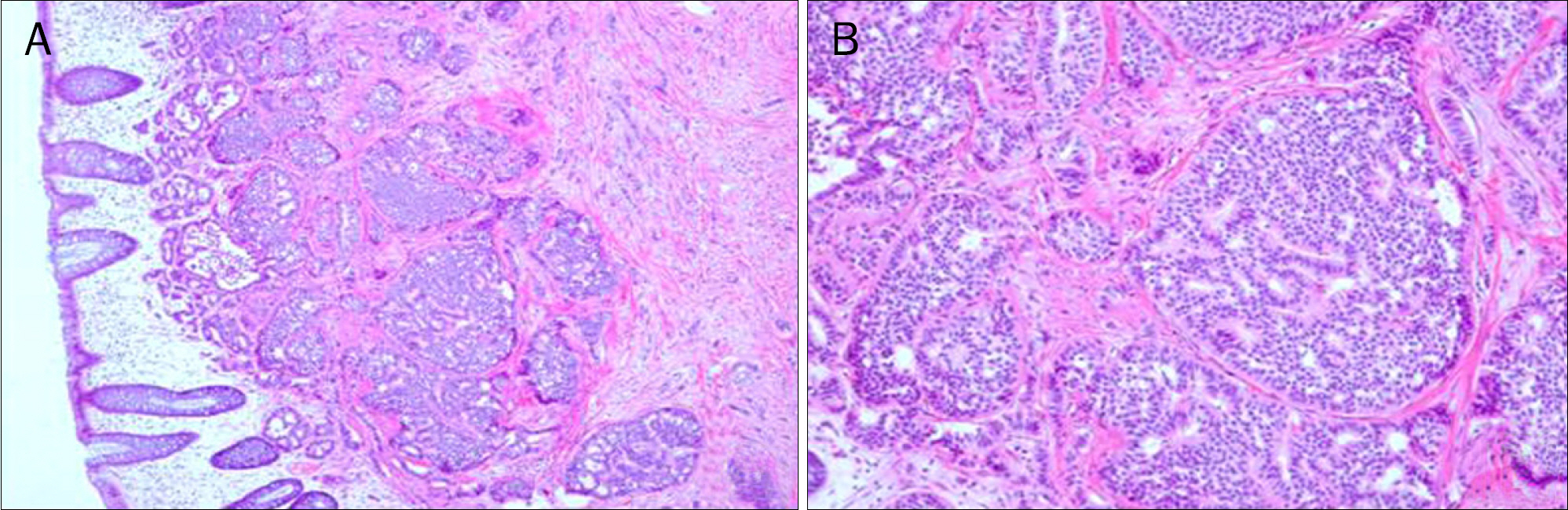
Fig. 5. Pathologic findings. (A) Carcinoid tumor is arising from lamina propria and infiltrating to submucosa (H&E, ×40). (B) Tumor cells forming the nesting pattern of growth (H&E, ×100).
Reference
-
References
1. Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO classification of tumours of the digestive system. 4th ed.Lyon: IARC;2010.2. Teleky B, Herbst F, Längle F, Neuhold N, Niederle B. The prognosis of rectal carcinoid tumours. Int J Colorectal Dis. 1992; 7:11–14.
Article3. Memon MA, Nelson H. Gastrointestinal carcinoid tumors: current management strategies. Dis Colon Rectum. 1997; 40:1101–1118.4. Northrop JA, Lee JH. Large bowel carcinoid tumors. Curr Opin Gastroenterol. 2007; 23:74–78.
Article5. Naunheim KS, Zeitels J, Kaplan EL, et al. Rectal carcinoid tumors–treatment and prognosis. Surgery. 1983; 94:670–676.6. Chang JH, Kim SW, Chung WC, et al. Clinical review of gastrointestinal carcinoid tumor and analysis of the factors predicting metastasis. Korean J Gastroenterol. 2007; 50:19–25.7. Jung KC, Kim HS, Song SY, Choe GY, Kim YI. Carcinoid tumors of the gastrointestinal tract: analysis of 36 cases. Korean J Pathol. 1996; 30:396–407.8. Scherübl H. Rectal carcinoids are on the rise: early detection by screening endoscopy. Endoscopy. 2009; 41:162–165.
Article9. Saha S, Hoda S, Godfrey R, Sutherland C, Raybon K. Carcinoid tumors of the gastrointestinal tract: a 44-year experience. South Med J. 1989; 82:1501–1505.10. Sasou S, Suto T, Satoh T, Tamura G, Kudara N. Multiple carcinoid tumors of the rectum: report of two cases suggesting the origin of carcinoid tumors. Pathol Int. 2012; 62:699–703.
Article11. Haraguchi M, Kinoshita H, Koori M, et al. Multiple rectal carcinoids with diffuse ganglioneuromatosis. World J Surg Oncol. 2007; 5:19.
Article12. Kim WS, Choi SL, Song DJ, et al. Two cases of multiple carcinoid tumors of the rectum. Korean J Gastrointest Endosc. 2001; 23:192–196.13. Cha JM, Lee JI, Choe JW, et al. A case of multiple carcinoid tumors of the rectum. Korean J Gastrointest Endosc. 2008; 37:132–136.14. Burke AP, Thomas RM, Elsayed AM, Sobin LH. Carcinoids of the jejunum and ileum: an immunohistochemical and clinicopathologic study of 167 cases. Cancer. 1997; 79:1086–1093.15. Mashimo Y, Matsuda T, Uraoka T, et al. Endoscopic submucosal resection with a ligation device is an effective and safe treatment for carcinoid tumors in the lower rectum. J Gastroenterol Hepatol. 2008; 23:218–221.
Article16. Kim HH, Park SJ, Lee SH, et al. Efficacy of endoscopic submucosal resection with a ligation device for removing small rectal carcinoid tumor compared with endoscopic mucosal resection: analysis of 100 cases. Dig Endosc. 2012; 24:159–163.
Article17. Saito T, Ikenaga M, Yasui M, et al. A case of 7 mm rectal carcinoid with lymph node metastasis. Gan To Kagaku Ryoho. 2009; 36:2251–2253.18. Akasu T, Moriya Y, Sugihara K. Transrectal ultrasonography of a small rectal carcinoid tumor with lymph node metastasis: a case report. Jpn J Clin Oncol. 1996; 26:112–115.
Article19. Baik DS, Lee JH, Lee SI, Shin JE, Park SW, Lee WA. A small rectal carcinoid tumor with multiple liver metastases. Korean J Gastrointest Endosc. 2007; 34:233–238.20. Jeen YT, Chun HJ, Lee SJ, et al. The clinical value of endoscopic ultrasonography (EUS) in rectal carcinoid tumor. Korean J Gastrointest Endosc. 2000; 21:774–779.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Low-grade Rectal Neuroendocrine Tumor Recurring as Multiple Hepatic Metastasis after Complete Endoscopic Removal: A Case Report
- Endoscopic Treatment Outcome of Rectal Neuroendocrine Tumors Removed by Ligation-assisted Endoscopic Submucosal Resection
- Multiple Neuroendocrine Tumors in Stomach and Duodenum in a Multiple Endocrine Neoplasia Type 1 Patient
- Neuroendocrine Tumors of the Female Reproductive Tract: A Literature Review
- Proper Treatment Option for Small Rectal Neuroendocrine Tumors Using Precut Endoscopic Mucosal Resection
