Korean J Perinatol.
2015 Dec;26(4):365-368. 10.14734/kjp.2015.26.4.365.
Prenatal Diagnosis of Fetal Goiter in a Euthyroid Mother
- Affiliations
-
- 1Department of Obstetrics and Gynecology, School of Medicine, Catholic University of Daegu, Korea. magu815@cu.ac.kr
- 2Department of Pediatrics, School of Medicine, Catholic University of Daegu, Korea.
- KMID: 2164195
- DOI: http://doi.org/10.14734/kjp.2015.26.4.365
Abstract
- Congenital fetal goiter is a very rare pathology, is sometimes difficult to diagnose when there is no maternal history or the goiter size is moderate. We report a case of prenatally diagnosed fetal goiter in a euthyroid mother. A 28-year-old woman was referred to our clinic at 38(+2) weeks of gestation. Ultrasonographic examination revealed a fetal goiter. The maternal history and thyroid function tests, including antithyroid autoantibody tests, were unremarkable. Cesarean section was performed, and the thyroid profile of the neonate was consistent with congenital hypothyroidism. Thyroxine therapy was immediately started. Fetal thyroid function must be determined when a goiter is detected. Cordocentesis is a more reliable but riskier diagnostic tool than amniocentesis. Intra-amniotic injection of thyroxine is relatively safe and an easier management option for fetal hypothyroidism. To develop more noninvasive and safe methods for therapeutic efficacy monitoring, a large-scale study is necessary.
MeSH Terms
Figure
-

Fig. 1. Sagittal ultrasonogram shows a symmetrical bilobed mass measuring 34.4×17.4 mm at the anterior portion of the fetal neck.
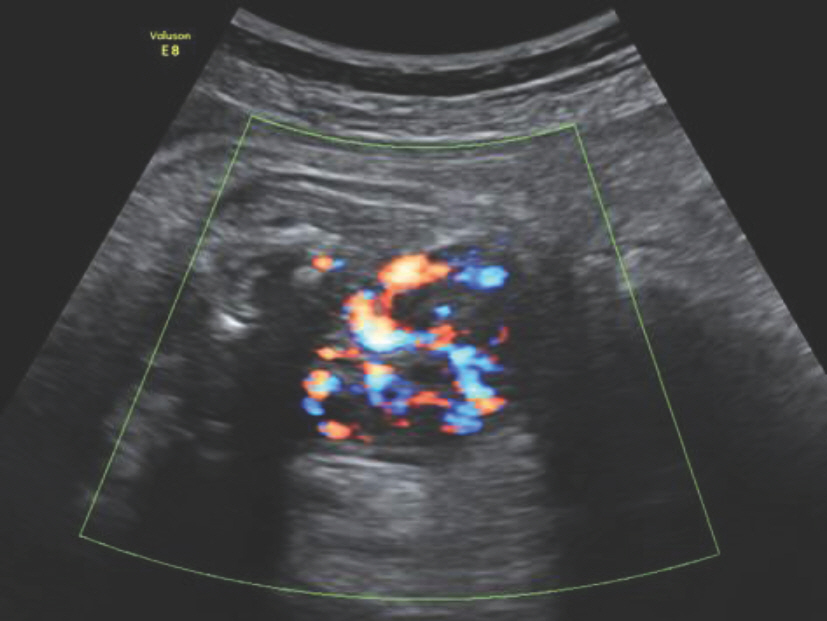
Fig. 2. Sagittal ultrasonogram of the fetal neck shows a goiter with peripheral flushing.
Reference
-
References
1. Blumenfeld YJ, Davis A, Milan K, Chueh J, Hudgins L, Barth RA, et al. Conservatively managed fetal goiter: an alternative to in utero therapy. Fetal Diagn Ther. 2013; 34:184–7.
Article2. Göktolga U, Karaşahin KE, Gezginç K, Fidan U, Ergün A, Başer I. Intrauterine fetal goiter: diagnosis and management. Taiwan J Obstet Gynecol. 2008; 47:87–90.
Article3. Koyuncu FM, Tamay AG, Bugday S. Intrauterine diagnosis and management of fetal goiter: a case report. J Clin Ultrasound. 2010; 38:503–5.
Article4. Stewart CJ, Constantatos S, Joolay Y, Muller L. In utero treatment of fetal goitrous hypothyroidism in a euthyroid mother: a case report. J Clin Ultrasound. 2012; 40:603–6.
Article5. Uhrmann S, Marks KH, Maisels MJ, Kulin HE, Kaplan M, Utiger R. Frequency of transient hypothyroxinaemia in low birthweight infants. Potential pitfall for neonatal screening programmes. Arch Dis Child. 1981; 56:214–7.
Article6. Haddow JE, Palomaki GE, Allan WC, Williams JR, Knight GJ, Gagnon J, et al. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med. 1999; 341:549–55.
Article7. Rovet J, Daneman D. Congenital hypothyroidism: a review of current diagnostic and treatment practices in relation to neuropsychologic outcome. Paediatr Drugs. 2003; 5:141–9.8. Song SI, Daneman D, Rovet J. The influence of etiology and treatment factors on intellectual outcome in congenital hypothyroidism. J Dev Behav Pediatr. 2001; 22:376–84.
Article9. Ho SS, Metreweli C. Normal fetal thyroid volume. Ultrasound Obstet Gynecol. 1998; 11:118–22.
Article10. Volumenie JL, Polak M, Guibourdenche J, Oury JF, Vuillard E, Sibony O, et al. Management of fetal thyroid goitres: a report of 11 cases in a single perinatal unit. Prenat Diagn. 2000; 20:799–806.
Article11. Hollingsworth DR, Alexander NM. Amniotic fluid concentrations of iodothyronines and thyrotropin do not reliably predict fetal thyroid status in pregnancies complicated by maternal thyroid disorders or anencephaly. J Clin Endocrinol Metab. 1983; 57:349–55.
Article12. Simsek M, Mendilcioglu I, Mihci E, Karaguzel G, Taskin O. Prenatal diagnosis and early treatment of fetal goitrous hypothyroidism and treatment results with two-year followup. J Matern Fetal Neonatal Med. 2007; 20:263–5.13. Agrawal P, Ogilvy-Stuart A, Lees C. Intrauterine diagnosis and management of congenital goitrous hypothyroidism. Ultrasound Obstet Gynecol. 2002; 19:501–5.
Article14. Corbacioglu Esmer A, Gul A, Dagdeviren H, Turan Bakirci I, Sahin O. Intrauterine diagnosis and treatment of fetal goitrous hypothyroidism. J Obstet Gynaecol Res. 2013; 39:720–3.
Article15. Mastrolia SA, Mandola A, Mazor M, Hershkovitz R, Mesner O, Beer-Weisel R, et al. Antenatal diagnosis and treatment of hypothyroid fetal goiter in an euthyroid mother: a case report and review of literature. J Matern Fetal Neonatal Med. 2015; 28:2214–20.
Article16. Hanono A, Shah B, David R, Buterman I, Roshan D, Shah S, et al. Antenatal treatment of fetal goiter: a therapeutic challenge. J Matern Fetal Neonatal Med. 2009; 22:76–80.
Article17. Huel C, Guibourdenche J, Vuillard E, Ouahba J, Piketty M, Oury JF, et al. Use of ultrasound to distinguish between fetal hyperthyroidism and hypothyroidism on discovery of a goiter. Ultrasound Obstet Gynecol. 2009; 33:412–20.
Article18. Shoham I, Aricha-Tamir B, Weintraub AY, Mazor M, Wiznitzer A, Holcberg G, et al. Fetal heart rate tracing patterns associated with congenital hypothyroidism. Am J Obstet Gynecol. 2009; 201:48.e1–4.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Prenatal Diagnosis of Congenital Fetal Goiter in Hyperthyroidism Mother
- Fetal goiter conservatively monitored during the prenatal period associated with maternal and neonatal euthyroid status
- Erratum: Prenatal Diagnosis of Fetal Goiter in a Euthyroid Mother
- Two Cases of Fetal Arachnoid Cyst Diagnosed by Prenatal Ultrasonography
- Relationship of Prenatal Stress and Depression to Maternal-Fetal Attachment and Fetal Growth
