Korean J Perinatol.
2015 Dec;26(4):289-298. 10.14734/kjp.2015.26.4.289.
Minimally Invasive Surfactant Therapy
- Affiliations
-
- 1Department of Pediatrics, Inje University Sanggye Paik Hospital, Seoul, Korea. peddoc@paik.ac.kr
- KMID: 2164183
- DOI: http://doi.org/10.14734/kjp.2015.26.4.289
Abstract
- For many years preterm infants with respiratory distress syndrome have been managed with a combination of intubation and surfactant replacement therapy. It is now recognized that applying noninvasive ventilation (NIV) such as nasal continuous positive airway pressure (CPAP) in preterm infants is a reasonable alternative to early intubation after birth. Recently, nasal CPAP has shown a benefit with a small reduction in the risk of the combined outcome of death or bronchopulmonary dysplasia. There has been an upsurge in the use of NIV as primary therapy for preterm infants, bringing with it the dilemma of when and how to give exogenous surfactant. In an effort to overcome this problem, minimally invasive surfactant therapy (MIST) to spontaneously breathing infants, allows them to remain on CPAP in first days after birth. MIST has included administration of exogenous surfactant by brief tracheal catheterization, aerosolization, laryngeal mask, and intrapharyngeal instillation. In recent clinical trials, surfactant delivery via brief tracheal catheterization was found to reduce the need for subsequent intubation and mechanical ventilation and to improve short-term respiratory outcomes. In conclusion, MIST is gentle, safe, feasible and effective to perform in preterm infants and will also be used commonly in Korea.
Keyword
MeSH Terms
Figure
-

Fig. 1. Cologne methods of tracheal catheterization for surfactant replacement therapy. (A) Equipment of Cologne method is shown (feeding tube, 10 mL syringe, Magill's forceps, and laryngoscope with blade). Insertion of the feeding tube (B) and administration of surfactant (C) are shown.
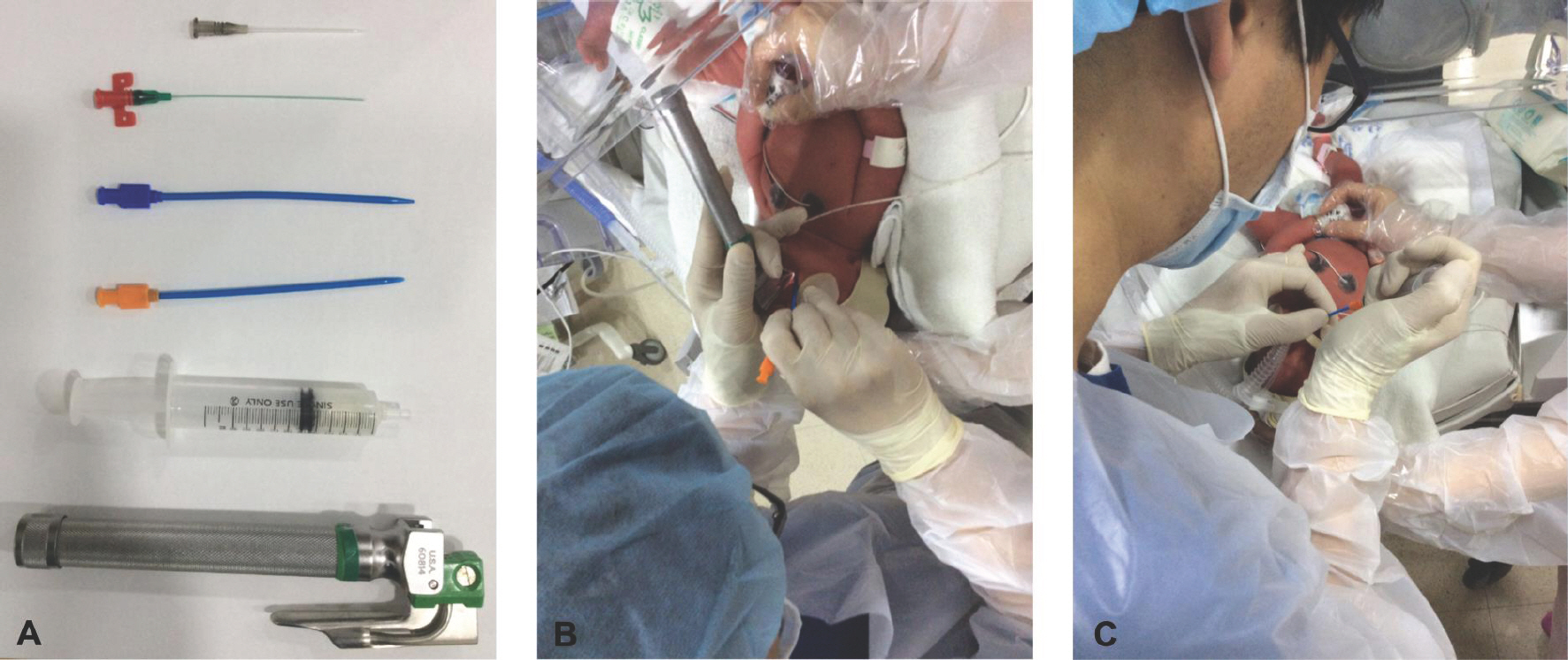
Fig. 2. Hobart methods of tracheal catheterization for surfactant replacement therapy. (A) Equipment of Hobart method is shown (vascular catheters, 10 mL syringe, and laryngoscope with blade). Insertion of the vascular catheter (B) and administration of surfactant (C) are shown.
Reference
-
References
1. Yost CC, Soll RF. Early versus delayed selective surfactant treatment for neonatal respiratory distress syndrome. Cochrane Database Syst Rev. 1999; 4:CD001456.2. Soll RF, Morley CJ. Prophylactic versus selective use of surfactant in preventing morbidity and mortality in preterm infants. Cochrane Database Syst Rev. 2001; 2:CD000510.
Article3. Iliodromiti Z, Zygouris D, Sifakis S, Pappa KI, Tsikouras P, Salakos N, et al. Acute lung injury in preterm fetuses and neonates: mechanisms and molecular pathways. J Matern Fetal Neonatal Med. 2013; 26:1696–704.
Article4. Chowdhury O, Wedderburn CJ, Duffy D, Greenough A. CPAP review. Eur J Pediatr. 2012; 171:1441–8.
Article5. Kjellberg M, Bjorkman K, Rohdin M, Sanchez-Crespo A, Jonsson B. Bronchopulmonary dysplasia: Clinical grading in relation to ventilation/perfusion mismatch measured by single photon emission computed tomography. Pediatr Pulmonol. 2013; 48:1206–13.
Article6. Hillman N, Jobe AH. Noninvasive strategies for management of respiratory problems in neonates. NeoReviews. 2013; 14:227–36.
Article7. Dargaville P, Aiyappan A, De Paoli AG, Dalton RG, Kuschel CA, Kamlin CO, et al. Continuous positive airway pressure failure in preterm infants: incidence, predictors and consequences. Neonatology. 2013; 104:8–14.
Article8. Verder H. Surfactant therapy and nasal continuous positive airway pressure for newborns with respiratory distress syndrome. N Engl J Med. 1994; 331:1051–5.
Article9. Verder H, Albertsen P, Ebbesen F, Greisen G, Robertson B, Bertelsen A, et al. Nasal continuous positive airway pressure and early surfactant therapy for respiratory distress syndrome in newborns of less than 30 weeks'gestation. Pediatrics. 1999; 103:E24.10. Bohlin K, Henckel E, Blennow M. International perspectives: Surfactant without assisted ventilation: the Scandinavian perspective. NeoReviews. 2008; 9:555–61.11. Venkatesh V. Endotracheal intubation in a neonatal population remains associated with a high risk of adverse effects. Eur J Pediatr. 2011; 170:223–7.12. Nilsson R, Grossmann G, Robertson B. Bronchiolar epithelial lesions induced in the premature rabbit neonate by short periods of artificial ventilation. Acta Pathol Microbiol Scand A. 1980; 88:359–67.
Article13. Kolatat T. Airway complications in neonates who received mechanical ventilation. J Med Assoc Thai. 2002; 85:S455–62.14. Allen K. Premedication for neonatal intubation. Adv Neon Care. 2011; 12:107–11.
Article15. Aguar M, Vento M, Dargaville PA. Minimally invasive surfactant therapy: an update. NeoReviews. 2014; 15:275–85.
Article16. Kattwinkel J, Robinson M, Bloom BT, Delmore P, Ferguson JE. Technique for intrapartum administration of surfactant without requirement for an endotracheal tube. J Perinatol. 2004; 24:360–5.
Article17. Kribs A, Pillekamp F, Hünseler C, Vierzig A, Roth B. Early administration of surfactant in spontaneous breathing with nCPAP: feasibility and outcome in extremely premature infants (postmenstrual age </=27 weeks). Paediatr Anaesth. 2007; 17:364–9.18. Trevisanuto D, Grazzina N, Ferrarese P, Micaglio M, Verghese C, Zanardo V. Laryngeal mask airway used as a delivery conduit for the administration of surfactant to preterm infants with respiratory distress syndrome. Biol Neonate. 2005; 87:217–20.
Article19. Berggren E, Liljedahl M, Winbladh B, Andreasson B, Curstedt T, Robertson B, et al. Pilot study of nebulized surfactant therapy for neonatal respiratory distress syndrome. Acta Paediatr. 2000; 89:460–4.
Article20. Kribs A, Vierzig A, Hünseler C, Eifinger F, Welzing L, Stützer H, et al. Early surfactant in spontaneously breathing with nCPAP in ELBW infants – a single centre four year experience. Acta Paediatr. 2008; 97:293–8.
Article21. Dargaville P. Innovation in surfactant therapy I: surfactant lavage and surfactant administration by fluid bolus using minimally invasive techniques. Neonatology. 2012; 101:326–36.
Article22. Enhörning G, Robertson B. Lung expansion in the premature rabbit fetus after tracheal deposition of surfactant. Pediatrics. 1972; 50:58–66.23. Ten Centre Study Group. Ten Centre Trial of artificial surfactant (artificial lung expanding compound) in very premature babies. Br Med J (Clin Res Ed). 1987; 294:991–6.24. Dambeanu JM, Parmigiani S, Marinescu B, Bevilacqua G. Use of surfactant for prevention of respiratory distress syndrome in newborn infants in spontaneous breathing: a randomized multicenter clinical pilot-study. Acta Biomed Ateneo Parmense. 1997; 68(Suppl 1):39–45.25. Abdel-Latif ME, Osborn DA: Pharyngeal instillation of surfactant before the first breath for prevention of morbidity and mortality in preterm infants at risk of respiratory distress syndrome. Cochrane Database Syst Rev. 2011; 3:CD008311.26. Verder H, Agertoft L, Albertsen P, Christensen NC, Curstedt T, Ebbesen F, et al. Surfactant treatment of newborn infants with respiratory distress syndrome primarily treated with nasal continuous positive air pressure. A pilot study. Ugeskr Laeger. 1992; 154:2136–9.27. Dargaville P, Aiyappan A, Cornelius A, Williams C, De Paoli AG. Preliminary evaluation of a new technique of minimally invasive surfactant therapy. Arch Dis Child Fetal Neonatal Ed. 2011; 96:F243–8.
Article28. Dargaville P, Aiyappan A, De Paoli AG, Kuschel CA, Kamlin CO, Carlin JB, et al. Minimally invasive surfactant therapy in preterm infants on continuous positive airway pressure. Arch Dis Child Fetal Neonatal Ed. 2013; 98:F122–6.29. Kanmaz HG, Erdeve O, Canpolat FE, Mutlu B, Dilmen U. Surfactant administration via thin catheter during spontaneous breathing: randomized controlled trial. Pediatrics. 2013; 131:e502–9.
Article30. Aguar M, Cernada M, Brugada M, Gimeno A, Gutierrez A, Vento M. Minimally invasive surfactant therapy with a gastric tube is as effective as the intubation, surfactant, and extubation technique in preterm babies. Acta Paediatr. 2014; 103:e229–33.
Article31. Kribs A, H¨artel C, Kattner E, Vochem M, Küster H. Surfactant without intubation in preterm infants with respiratory distress: first multicenter data. Klin Paediatr. 2010; 222:13–7.
Article32. Jorch G, Hartl H, Roth B, Kribs A, Gortner L, Schaible T, et al. Surfactant aerosol treatment of respiratory distress syndrome in spontaneously breathing premature infants. Pediatr Pulmonol. 1997; 24:222–4.33. Lopez E, Gascoin G, Flamant C, Merhi M, Tourneux P, Baud O. French Young Neonatologist Club. Exogenous surfactant therapy in 2013: what is next? Who, when and how should we treat newborn infants in the future? BMC Pediatr. 2013; 13:165.
Article34. Mazela J, Merritt TA, Finer NN. Aerosolized surfactants. Curr Opin Pediatr. 2007; 19:155–62.
Article35. Pillow JJ, Minocchieri S. Innovation in surfactant therapy II: surfactant administration by aerosolization. Neonatology. 2012; 101:337–44.
Article36. Attridge JT, Stewart C, Stukenborg GJ, Kattwinkel J. Administration of rescue surfactant by laryngeal mask airway: lessons from a pilot trial. Am J Perinatol. 2013; 30:201–6.37. More K, Sakhuja P, Shah PS. Minimally invasive surfactant administration in preterm infants: a meta-narrative review. JAMA Pediatr. 2014; 168:901–8.38. Göpel W, Kribs A, Ziegler A, Laux R, Hoehn T, Wieg C, et al. Avoidance of mechanical ventilation by surfactant treatment of spontaneously breathing preterm infants (AMV): an open-label, randomised, controlled trial. Lancet. 2011; 378:1627–34.
Article39. Klebermass-Schrehof K, Wald M, Schwindt J, Grill A, Prusa AR, Haiden N, et al. Less invasive surfactant administration in extremely preterm infants: impact on mortality and morbidity. Neonatology. 2013; 103:252–8.
Article40. Kribs A, Roll C, Göpel W, Wieg C, Groneck P, Laux R, et al. Nonintubated surfactant application vs conventional therapy in extremely preterm infants: a randomized clinical trial. JAMA Pediatr. 2015; 169:723–30.41. Göpel W, Kribs A, Härtel C, Avenarius S, Teig N, Groneck P, et al. Less invasive surfactant administration is associated with improved pulmonary outcomes in spontaneously breathing preterm infants. Acta Paediatr. 2015; 104:241–6.
Article42. Mohammadizadeh M, Ardestani AG, Sadeghnia AR. Early administration of surfactant via a thin intratracheal catheter in preterm infants with respiratory distress syndrome: Feasibility and outcome. J Res Pharm Pract. 2015; 4:31–6.
Article43. Bao Y, Zhang G, Wu M, Ma L, Zhu J. A pilot study of less invasive surfactant administration in very preterm infants in a Chinese tertiary center. BMC Pediatr. 2015; 15:21.
Article44. Herting E. Less invasive surfactant administration (LISA) – ways to deliver surfactant in spontaneously breathing infants. Early Hum Dev. 2013; 89:875–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of minimally invasive surfactant therapy with intubation surfactant administration and extubation for treating preterm infants with respiratory distress syndrome: a randomized clinical trial
- A New Beginning for the Journal of Minimally Invasive Surgery for the International Recognition and Contribution of Scientific Development of Minimally Invasive Surgery
- Clinical Outcomes of Minimally Invasive Surfactant Therapy via Tracheal Catheterization in Neonates with a Gestational Age of 30 Weeks or More Diagnosed with Respiratory Distress Syndrome
- Update of minimally invasive surfactant therapy
- Establishment of Minimally Invasive Thoracic Surgery Program
