Yonsei Med J.
2015 Sep;56(5):1401-1407. 10.3349/ymj.2015.56.5.1401.
Risk Assessment of Mortality Following Intraoperative Cardiac Arrest Using POSSUM and P-POSSUM in Adults Undergoing Non-Cardiac Surgery
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Seoul, Korea. koobn@yuhs.ac
- KMID: 2163636
- DOI: http://doi.org/10.3349/ymj.2015.56.5.1401
Abstract
- PURPOSE
The Physiological and Operative Severity Score for enUmeration of Mortality and morbidity (POSSUM) and its Portsmouth modification (P-POSSUM) are comprehensive assessment methods for evaluating patient and surgical factors widely used to predict 30-day mortality rates. In this retrospective study, we evaluated the usefulness of POSSUM and P-POSSUM in predicting 30-day mortality after intraoperative cardiac arrests in adult patients undergoing non-cardiac surgery.
MATERIALS AND METHODS
Among 190486 patients who underwent anesthesia, 51 experienced intraoperative cardiac arrest as defined in our study protocol. Predicted mortality rates were calculated using POSSUM and P-POSSUM equations and were compared with actual outcomes using exponential and linear analyses. In addition, a receiver operating characteristic curve analysis was undertaken, and area-under-the-curve (AUC) values with confidence intervals (CIs) were calculated for POSSUM and P-POSSUM.
RESULTS
Among the 51 patients with intraoperative cardiac arrest, 32 (62.7%) died within 30 days postoperatively. The overall predicted 30-day mortality rates using POSSUM and P-POSSUM were 65.5% and 57.5%, respectively. The observed-to-predicted (O:E) ratio for the POSSUM 30-day mortality was 1.07, with no significant difference between the observed and predicted values (chi2=4.794; p=0.779). P-POSSUM predicted mortality equally well, with an O:E ratio of 1.10 (chi2=8.905; p=0.350). AUC values (95% CI) were 0.771 (0.634-0.908) and 0.785 (0.651-0.918) for POSSUM and P-POSSUM, respectively.
CONCLUSION
Both POSSUM and P-POSSUM performed well to predict overall 30-day mortality following intraoperative cardiac arrest in adults undergoing non-cardiac surgery at a university teaching hospital in Korea.
Keyword
MeSH Terms
-
Adult
Aged
Female
Heart Arrest/*complications/mortality
Humans
Incidence
Intraoperative Complications/*mortality
Male
Middle Aged
Morbidity
Postoperative Period
ROC Curve
Republic of Korea/epidemiology
Retrospective Studies
Risk Assessment/*methods
*Severity of Illness Index
Surgical Procedures, Operative/*mortality
Figure
-
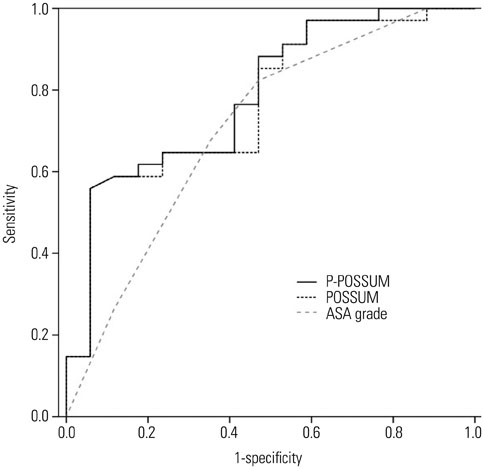
Fig. 1 Receiver operator characteristic curves for the POSSUM, P-POSSUM, and American Society of Anesthesiologists (ASA) grade in the prediction of 30-day mortality after intraoperative cardiac arrest. The areaunder-the-curve values with 95% confidence intervals were 0.771 (0.634-0.908), 0.785 (0.651-0.918), and 0.708 (0.549-0.866) for POSSUM, P-POSSUM, and ASA grade, respectively. POSSUM, Physiological and Operative Severity Score for enUmeration of Mortality and morbidity; P-POSSUM, Portsmouth modification POSSUM.
Reference
-
1. Goswami S, Brady JE, Jordan DA, Li G. Intraoperative cardiac arrests in adults undergoing noncardiac surgery: incidence, risk factors, and survival outcome. Anesthesiology. 2012; 117:1018–1026.2. Sprung J, Warner ME, Contreras MG, Schroeder DR, Beighley CM, Wilson GA, et al. Predictors of survival following cardiac arrest in patients undergoing noncardiac surgery: a study of 518,294 patients at a tertiary referral center. Anesthesiology. 2003; 99:259–269.
Article3. Newland MC, Ellis SJ, Lydiatt CA, Peters KR, Tinker JH, Romberger DJ, et al. Anesthetic-related cardiac arrest and its mortality: a report covering 72,959 anesthetics over 10 years from a US teaching hospital. Anesthesiology. 2002; 97:108–115.4. Ramachandran SK, Mhyre J, Kheterpal S, Christensen RE, Tallman K, Morris M, et al. Predictors of survival from perioperative cardiopulmonary arrests: a retrospective analysis of 2,524 events from the Get With The Guidelines-Resuscitation registry. Anesthesiology. 2013; 119:1322–1339.5. Chan PS, Spertus JA, Krumholz HM, Berg RA, Li Y, Sasson C, et al. A validated prediction tool for initial survivors of in-hospital cardiac arrest. Arch Intern Med. 2012; 172:947–953.
Article6. Aschauer S, Dorffner G, Sterz F, Erdogmus A, Laggner A. A prediction tool for initial out-of-hospital cardiac arrest survivors. Resuscitation. 2014; 85:1225–1231.
Article7. Poldermans D, Bax JJ, Boersma E, De Hert S, Eeckhout E, Fowkes G, et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery: the Task Force for Preoperative Cardiac Risk Assessment and Perioperative Cardiac Management in Non-cardiac Surgery of the European Society of Cardiology (ESC) and endorsed by the European Society of Anaesthesiology (ESA). Eur J Anaesthesiol. 2010; 27:92–137.
Article8. Copeland GP, Jones D, Walters M. POSSUM: a scoring system for surgical audit. Br J Surg. 1991; 78:355–360.
Article9. Whiteley MS, Prytherch DR, Higgins B, Weaver PC, Prout WG. An evaluation of the POSSUM surgical scoring system. Br J Surg. 1996; 83:812–815.
Article10. Neary WD, Heather BP, Earnshaw JJ. The Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity (POSSUM). Br J Surg. 2003; 90:157–165.
Article11. Wijesinghe LD, Mahmood T, Scott DJ, Berridge DC, Kent PJ, Kester RC. Comparison of POSSUM and the Portsmouth predictor equation for predicting death following vascular surgery. Br J Surg. 1998; 85:209–212.
Article12. Chen T, Wang H, Wang H, Song Y, Li X, Wang J. POSSUM and P-POSSUM as predictors of postoperative morbidity and mortality in patients undergoing hepato-biliary-pancreatic surgery: a metaanalysis. Ann Surg Oncol. 2013; 20:2501–2510.
Article13. Dutta S, Horgan PG, McMillan DC. POSSUM and its related models as predictors of postoperative mortality and morbidity in patients undergoing surgery for gastro-oesophageal cancer: a systematic review. World J Surg. 2010; 34:2076–2082.
Article14. Hobson SA, Sutton CD, Garcea G, Thomas WM. Prospective comparison of POSSUM and P-POSSUM with clinical assessment of mortality following emergency surgery. Acta Anaesthesiol Scand. 2007; 51:94–100.
Article15. Mohil RS, Bhatnagar D, Bahadur L, Rajneesh , Dev DK, Magan M. POSSUM and P-POSSUM for risk-adjusted audit of patients undergoing emergency laparotomy. Br J Surg. 2004; 91:500–503.
Article16. Neary WD, Prytherch D, Foy C, Heather BP, Earnshaw JJ. Comparison of different methods of risk stratification in urgent and emergency surgery. Br J Surg. 2007; 94:1300–1305.
Article17. Parmar CD, Torella F. Prediction of major adverse cardiac events in vascular surgery: are cardiac risk scores of any practical value? Vasc Endovascular Surg. 2010; 44:14–19.18. Donati A, Ruzzi M, Adrario E, Pelaia P, Coluzzi F, Gabbanelli V, et al. A new and feasible model for predicting operative risk. Br J Anaesth. 2004; 93:393–399.19. Ellis SJ, Newland MC, Simonson JA, Peters KR, Romberger DJ, Mercer DW, et al. Anesthesia-related cardiac arrest. Anesthesiology. 2014; 120:829–838.
Article20. Bennett-Guerrero E, Hyam JA, Shaefi S, Prytherch DR, Sutton GL, Weaver PC, et al. Comparison of P-POSSUM risk-adjusted mortality rates after surgery between patients in the USA and the UK. Br J Surg. 2003; 90:1593–1598.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- POSSUM, P-POSSUM, and Cr-POSSUM Scoring Systems as Predictors of Postoperative Morbidity and Mortality in Elderly Colorectal Cancer Patients
- A single emergency center study for evaluation of P-POSSUM and Mannheim Peritonitis Index as a risk prediction model in patients with non-traumatic peritonitis
- Evaluation of P-POSSUM as a Risk Prediction Model in Laparoscopic Gastrectomy of Elderly Patients with Gastric Cancer
- Validation of POSSUM-physiological Score as Predictors of Post-operative Morbidity and Mortality after Emergency Operation for Peptic Ulcer Complications
- Might simple peripheral blood parameters be an early indicator in the prediction of severity and morbidity of cholecystitis?
