Progression of periapical cystic lesion after incomplete endodontic treatment
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Yonsei University College of Dentistry, Seoul, Korea.
- 2Department of Conservative Dentistry, Oral Science Research Center, Yonsei University College of Dentistry, Seoul, Korea. sujungshin@yuhs.ac
- 3Department of Oral and Maxillofacial Radiology, Yonsei University College of Dentistry, Seoul, Korea.
- KMID: 2163296
- DOI: http://doi.org/10.5395/rde.2016.41.2.137
Abstract
- We report a case of large radicular cyst progression related to endodontic origin to emphasize proper intervention and follow-up for endodontic pathosis. A 25 yr old man presented with an endodontically treated molar with radiolucency. He denied any intervention because of a lack of discomfort. Five years later, the patient returned. The previous periapical lesion had drastically enlarged and involved two adjacent teeth. Cystic lesion removal and apicoectomy were performed on the tooth. Histopathological analysis revealed that the lesion was an inflammatory radicular cyst. The patient did not report any discomfort except for moderate swelling 3 days after the surgical procedure. Although the patient had been asymptomatic, close follow-ups are critical to determine if any periapical lesions persist after root canal treatment.
Figure
-
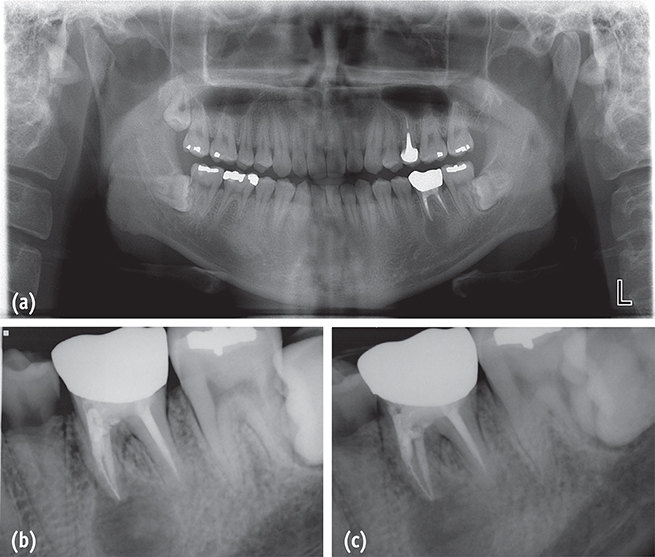
Figure 1 Initial radiograph findings when the patient first visited in 2009. (a) A panoramic radiograph revealed a periapical lesion on the mesial root of the left mandibular first molar (tooth #36); (b and c) Periapical radiographs showed radiolucency around the mesial root of tooth #36, and a metallic obstruction was noticed in one mesial canal.
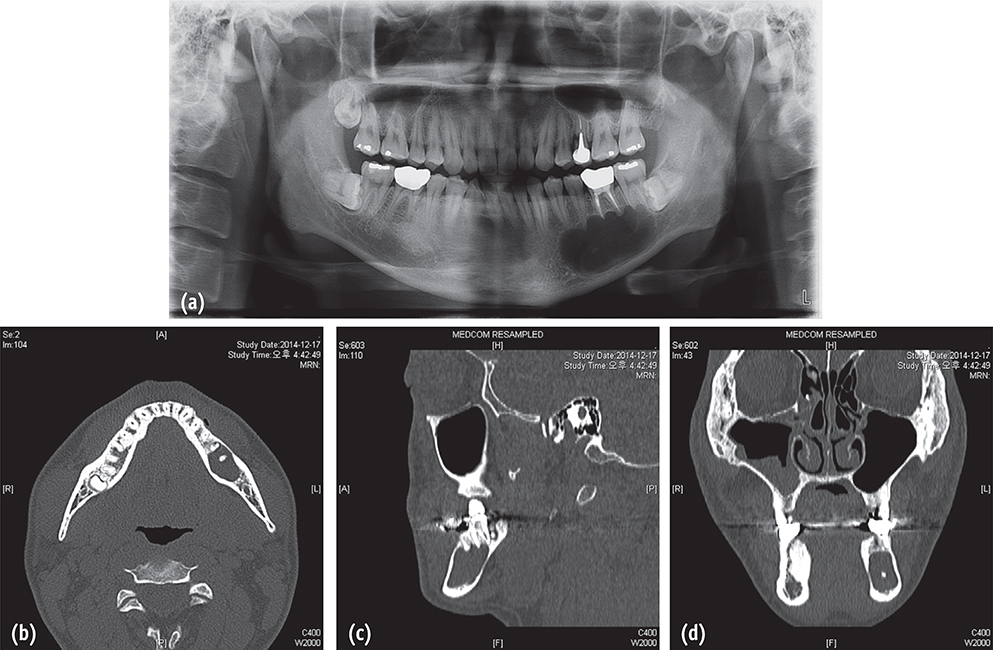
Figure 2 Radiographic findings in 2014. (a) A panoramic radiograph showed the progression of a cystic lesion around tooth #36, as compared to radiographs taken 5 years ago (Figure 1); (b and c) The computed tomography scan views demonstrated the thinning of the cortical plates on the buccal and lingual sides; (d) The coronal view showed a radiopaque material inside the lumen.
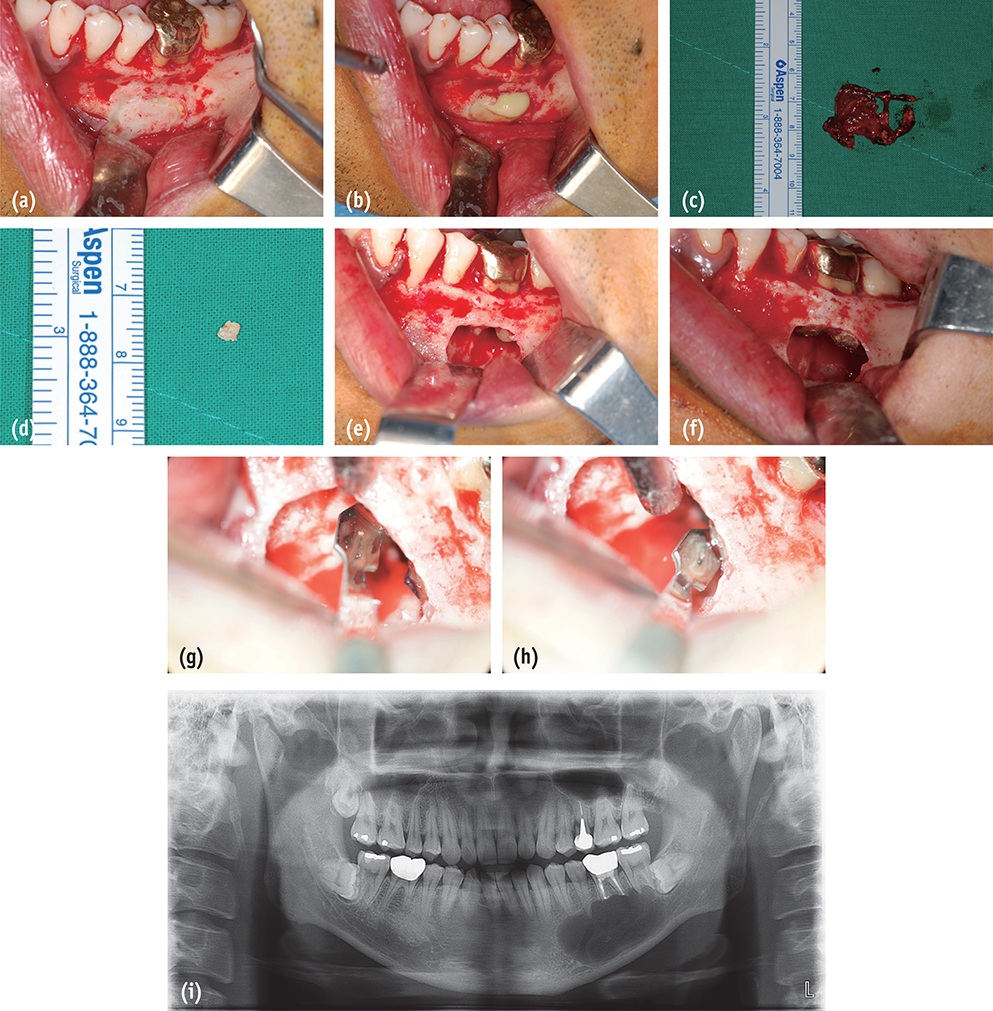
Figure 3 Clinical photos and a panoramic radiograph taken during the surgical procedure. (a) A bony window was prepared to save the cortical plate; (b) Pus-like turbid exudate from the lumen; (c) The cystic membrane was removed and sent for a biopsy; (d) A small, calcific material with a diameter of 3 mm was removed from the lumen; (e) An extruded endodontic file was observed in the mesial root; (f) Both roots were retrofilled with MTA. (g) The resected mesial root showed a metallic file in the mesiobuccal canal and leaked isthmus; (h) The resected distal root showed a filled canal with leakage; (i) Immediate postoperative panoramic radiograph.

Figure 4 Histology of the inflammatory radicular cyst. Hematoxylin and eosin stain. (a and b) Fibrous connective tissue lined with nonkeratinized epithelium (×40); (c) Cholesterol clefts (arrowheads) and inflammatory cells were found (×40).
Reference
-
1. Allard U, Palmqvist S. A radiographic survey of periapical conditions in elderly people in a Swedish county population. Endod Dent Traumatol. 1986; 2:103–108.
Article2. Eriksen HM, Bjertness E. Prevalence of apical periodontitis and results of endodontic treatment in middle-aged adults in Norway. Endod Dent Traumatol. 1991; 7:1–4.
Article3. Boucher Y, Matossian L, Rilliard F, Machtou P. Radiographic evaluation of the prevalence and technical quality of root canal treatment in a French subpopulation. Int Endod J. 2002; 35:229–238.
Article4. von Arx T, Roux E, Bürgin W. Treatment decisions in 330 cases referred for apical surgery. J Endod. 2014; 40:187–191.
Article5. Yu VS, Messer HH, Yee R, Shen L. Incidence and impact of painful exacerbations in a cohort with post-treatment persistent endodontic lesions. J Endod. 2012; 38:41–46.
Article6. Yu VS, Messer HH, Shen L, Yee R, Hsu CY. Lesion progression in post-treatment persistent endodontic lesions. J Endod. 2012; 38:1316–1321.
Article7. Santos SM, Soares JA, Costa GM, Brito-Júnior M, Moreira AN, de Magalhães CS. Radiographic parameters of quality of root canal fillings and periapical status: a retrospective cohort study. J Endod. 2010; 36:1932–1937.
Article8. Madras J, Lapointe H. Keratocystic odontogenic tumour: reclassification of the odontogenic keratocyst from cyst to tumour. J Can Dent Assoc. 2008; 74:165–165h.9. Estrela C, Decurcio DA, Silva JA, Mendonça EF, Estrela CR. Persistent apical periodontitis associated with a calcifying odontogenic cyst. Int Endod J. 2009; 42:539–545.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Non-surgical treatment of large periapical lesions
- The significance of diagnosis and treatment planning in periapical lesion overfilled with calcium hydroxide paste
- Prognostic factors influencing clinical outcome of nonsurgical endodontic treatment
- Necrosis of intact premolar caused by an adjacent apical infection: a case report
- The influence of periapical lesion on furcation involvement in mandibular molars
