IgG4-related disease of the rectum
- Affiliations
-
- 1Department of Surgery, Yeouido St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. wonkkang@catholic.ac.kr
- 2Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 3Department of Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2163070
- DOI: http://doi.org/10.4174/astr.2016.90.5.292
Abstract
- IgG4-related disease is a relatively new disease entity characterized by elevated serum IgG4 levels and marked infiltration of IgG4-positive plasma cells in lesions. Organ enlargement or nodular lesions consisting of abundant infiltration of lymphocytes and IgG4-positive plasma cells and fibrosis are seen in various organs throughout. We encountered a patient with an inflammatory pseudotumor of the rectum, which was histopathologically confirmed to be an IgG4-related disease. The patient was a 28-year-old woman who had constipation for 3 months. The endoluminal ultrasonography showed a lesion that was heterogeneous and low echogenic in lower rectum. The result of colonoscopic biopsy findings was of chronic proctitis with lymphoid aggregates. For a confirmative diagnosis, excision was performed. Histopathological examination represented plasma cell infiltration and fibrosis. Immunohistochemistry revealed prominence of IgG4-positive plasma cells and confirmed the diagnosis of IgG4-related disease. The patient is currently under observation on low-dose oral prednisolone without relapse.
Keyword
MeSH Terms
Figure
-

Fig. 1 Findings of imaging studies of IgG4-related disease of rectum. (A, B) Colonoscopic view of low rectum: 2-cm-sized protruding mass; (C) colonoscopic endoluminal ultrasonography view: 2-cm-sized heterogeneous low echogenic lesion involving mucosal, submucosal and proper muscle layer; (D) T1-weighted MRI. A 1.4-cm T1 low signal intensity mass (arrow) involving or abutting right anterior wall of lower rectum.
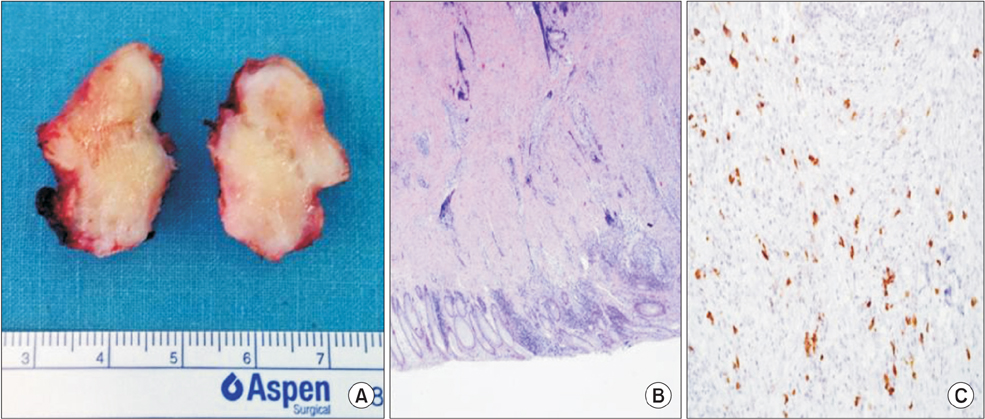
Fig. 2 Gross and histopathological features of IgG4-related disease of rectum. (A) Photograph of biopsy specimen; (B) tissue specimen from patient with IgG4-related disease shows rectum (H&E, ×100); (C) plasma cells in specimens (immunoperoxidase staining, ×100).
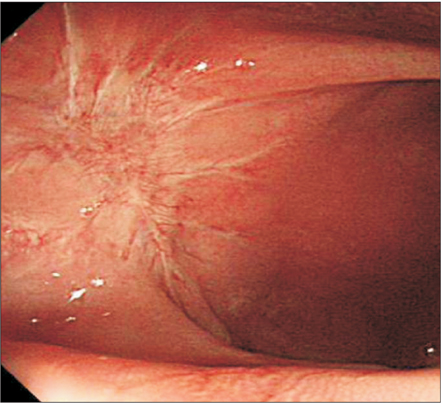
Fig. 3 Follow-up colonoscopic view of rectum: anal verge 4-cm healing state rectal wall.
Reference
-
1. Kamisawa T, Funata N, Hayashi Y, Eishi Y, Koike M, Tsuruta K, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol. 2003; 38:982–984.2. Kamisawa T, Takuma K, Egawa N, Tsuruta K, Sasaki T. Autoimmune pancreatitis and IgG4-related sclerosing disease. Nat Rev Gastroenterol Hepatol. 2010; 7:401–409.3. Research Committee to establish diagnostic criteria and development of treatment for systemic IgG4-related sclerosing disease. Research Committee to establish a new clinical entity, IgG4-related multiorgan lymphoproliferative syndrome (IgG4-MOLPS). Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD),2011. Research Program of Intractable Disease provided by the Ministry of Health, Labor, and Welfare of Japan. Nihon Naika Gakkai Zasshi. 2012; 101:795–804.4. Saeki T, Ito K, Yamazaki H, Imai N, Nishi S. Hypocomplementemia of unknown etiology: an opportunity to find cases of IgG4-positive multi-organ lymphoproliferative syndrome. Rheumatol Int. 2009; 30:99–103.5. Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001; 344:732–738.6. Hamano H, Kawa S, Ochi Y, Unno H, Shiba N, Wajiki M, et al. Hydronephrosis associated with retroperitoneal fibrosis and sclerosing pancreatitis. Lancet. 2002; 359:1403–1404.7. Hamano H, Arakura N, Muraki T, Ozaki Y, Kiyosawa K, Kawa S. Prevalence and distribution of extrapancreatic lesions complicating autoimmune pancreatitis. J Gastroenterol. 2006; 41:1197–1205.8. Zen Y, Fujii T, Harada K, Kawano M, Yamada K, Takahira M, et al. Th2 and regulatory immune reactions are increased in immunoglobin G4-related sclerosing pancreatitis and cholangitis. Hepatology. 2007; 45:1538–1546.9. Kamisawa T, Okamoto A. IgG4-related sclerosing disease. World J Gastroenterol. 2008; 14:3948–3955.10. Maruya S, Miura K, Tada Y, Masubuchi T, Nakamura N, Fushimi C, et al. Inflammatory pseudotumor of the parapharyngeal space: a case report. Auris Nasus Larynx. 2010; 37:397–400.
