Underestimated Sacroiliac Joint Lesion on Computed Tomography in Pelvic Open-book Injury: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Daejeon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Daejeon, Korea. ssewon@naver.com
- KMID: 2161315
- DOI: http://doi.org/10.5371/hp.2016.28.1.49
Abstract
- The classification of anteroposterior compression (APC) injury type is based on using static radiographs, stress radiographs are known as a useful adjunct in classifying type of APC pelvic injuries. According to a recent article, the intraoperative stress examination has led to a change in the treatment plan in more than 25% of patients on 22 patients presumed APC type I (symphyseal diastasis <2.5 cm) injuries. Here authors present a case demonstrating a necessity of intraoperative stress test for excluding concealed posterior ring disruption.
MeSH Terms
Figure
-
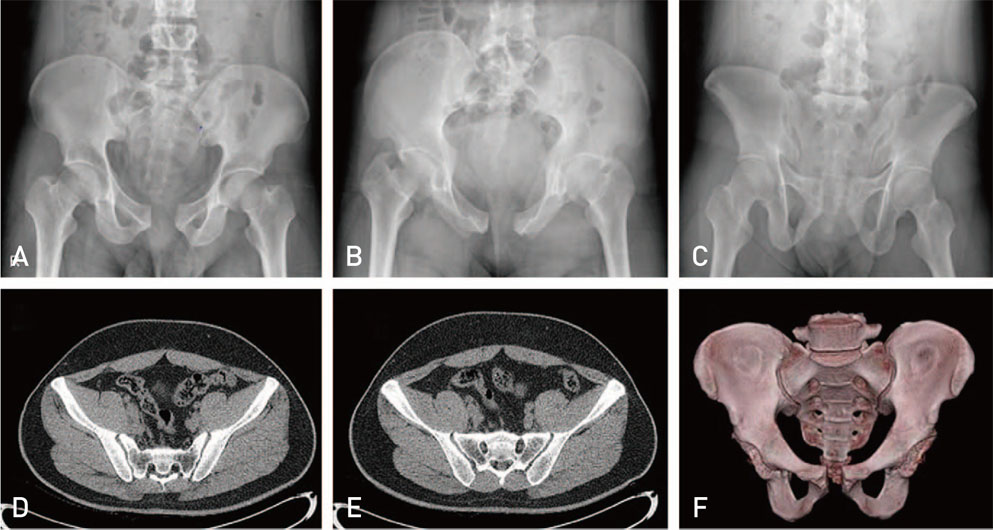
Fig. 1 Preoperative radiograph images showed 3.0-cm diastasis of pubic symphysis; pelvis anteroposterior (A), inlet (B), outlet view (C). Axial images (D, E) and three-dimensional image (F) of computed tomography (CT) revealed no diastasis of sacroiliac joint. Even if no pelvic manipulation has occurred, a static imaging like CT may lead to undersestimation of the actual injury.
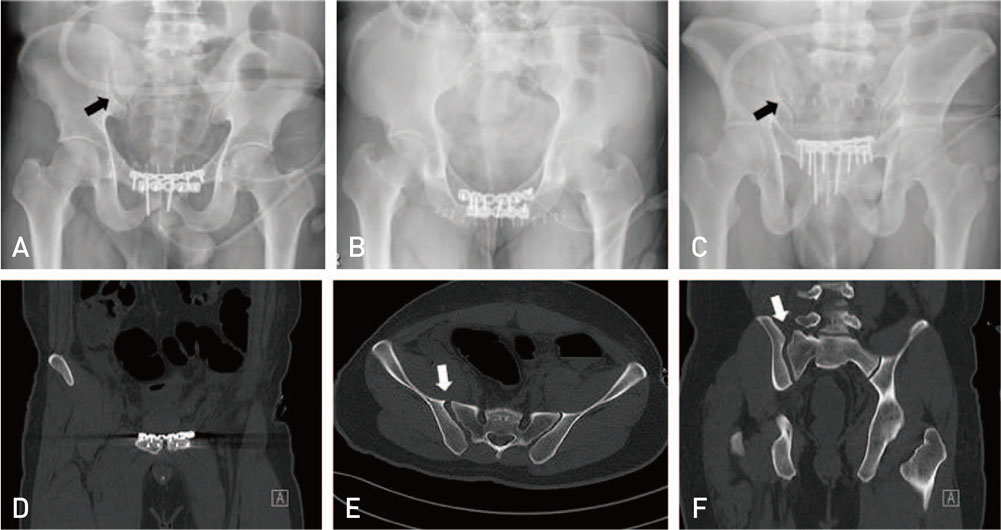
Fig. 2 After plating of pubic symphysis, right sacroiliac joint diastasis was observed; pelvis anteroposterior (A), inlet (B), outlet view (C). (D) Coronal computed tomography (CT) image of reduced pubic symphysis. (E) Axial and (F) coronal CT images of diastasis of right sacroiliac joint.
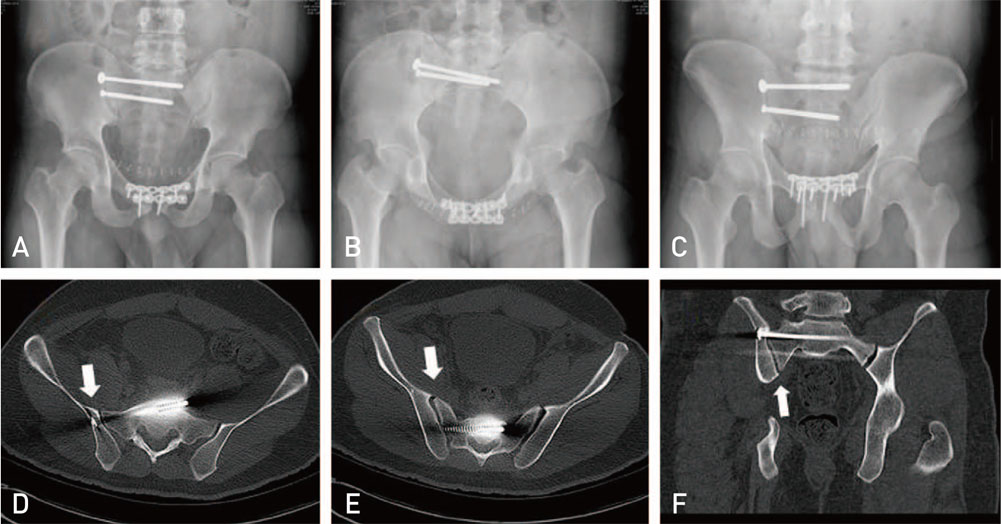
Fig. 3 After supplementary sacroiliac fixation, right sacroiliac joint diastasis was reduced; pelvis anteroposterior (A), inlet (B), outlet view (C). (D, E) Axial computed tomography (CT) images of reduced pubic symphysis. (F) Coronal CT image of diastasis of right sacroiliac joint.

Fig. 4 One year after injury follow-up radiographs; pelvis anteroposterior (A), inlet (B), outlet view (C). It showed no screw breakage, fixation failure or heterotopic ossification.
Reference
-
1. Burgess AR, Eastridge BJ, Young JW, et al. Pelvic ring disruptions: effective classification system and treatment protocols. J Trauma. 1990; 30:848–856.2. Oh KJ, Hwang SM. Surgical fixation of sacroiliac joint complex in unstable pelvic ring injuries. Hip Pelvis. 2012; 24:139–147.
Article3. Dujardin FH, Roussignol X, Hossenbaccus M, Thomine JM. Experimental study of the sacroiliac joint micromotion in pelvic disruption. J Orthop Trauma. 2002; 16:99–103.
Article4. Phieffer LS, Lundberg WP, Templeman DC. Instability of the posterior pelvic ring associated with disruption of the pubic symphysis. Orthop Clin North Am. 2004; 35:445–449.
Article5. Sagi HC, Papp S. Comparative radiographic and clinical outcome of two-hole and multi-hole symphyseal plating. J Orthop Trauma. 2008; 22:373–378.
Article6. Sagi HC, Ordway NR, DiPasquale T. Biomechanical analysis of fixation for vertically unstable sacroiliac dislocations with iliosacral screws and symphyseal plating. J Orthop Trauma. 2004; 18:138–143.
Article7. Suzuki T, Morgan SJ, Smith WR, Stahel PF, Flierl MA, Hak DJ. Stress radiograph to detect true extent of symphyseal disruption in presumed anteroposterior compression type I pelvic injuries. J Trauma. 2010; 69:880–885.
Article8. Nork S. The management of injured pelvic ring. In : Tile M, Helfet D, Kellam J, Vrahas M, editors. Fractures of the pelvis and acetabulum. 4th ed. Philadelphia: Lippincott Williams & Wilkins;2015. p. 159–174.9. Giannoudis PV, Chalidis BE, Roberts CS. Internal fixation of traumatic diastasis of pubic symphysis: is plate removal essential. Arch Orthop Trauma Surg. 2008; 128:325–331.
Article10. Simonian PT, Routt ML Jr, Harrington RM, Mayo KA, Tencer AF. Biomechanical simulation of the anteroposterior compression injury of the pelvis. An understanding of instability and fixation. Clin Orthop Relat Res. 1994; (309):245–256.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Computed Tomography in Pelvic Fracture
- Atypical Pelvic Crescent Fracture Caused by Vertical Shear Force
- Unilateral Ureteric Entrapment within the Sacroiliac Joint Causing Unilateral Hydroureteronephrosis
- Surgical Fixation of Sacroiliac Joint Complex in Unstable Pelvic Ring Injuries
- Pyomyositis of the iliacus muscle and pyogenic sacroiliitis after sacroiliac joint block: A case report
