Immunoglobulin G4-Related Kidney Disease: A Comprehensive Pictorial Review of the Imaging Spectrum, Mimickers, and Clinicopathological Characteristics
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul 05505, Korea. kimjhrad@amc.seoul.kr
- KMID: 2160773
- DOI: http://doi.org/10.3348/kjr.2015.16.5.1056
Abstract
- Immunoglobulin G4 (IgG4)-related kidney disease (IgG4-KD) has recently been demonstrated to be an important part of IgG4-related sclerosing disease (IgG4-SD). However, since IgG4-KD is still relatively unfamiliar to radiologists and physicians as compared to IgG4-SD involving other organs, it could, therefore, be easily missed. In this article, we present a comprehensive pictorial review of IgG4-KD with regards to the imaging spectrum, mimickers, and clinicopathologic characteristics, based on our clinical experience with 48 patients during the past 13 years, as well as a literature review. Awareness of the broad imaging spectrum of IgG4-KD and differential diagnosis from its mimickers will thus facilitate its early diagnosis and treatment.
Keyword
MeSH Terms
Figure
-
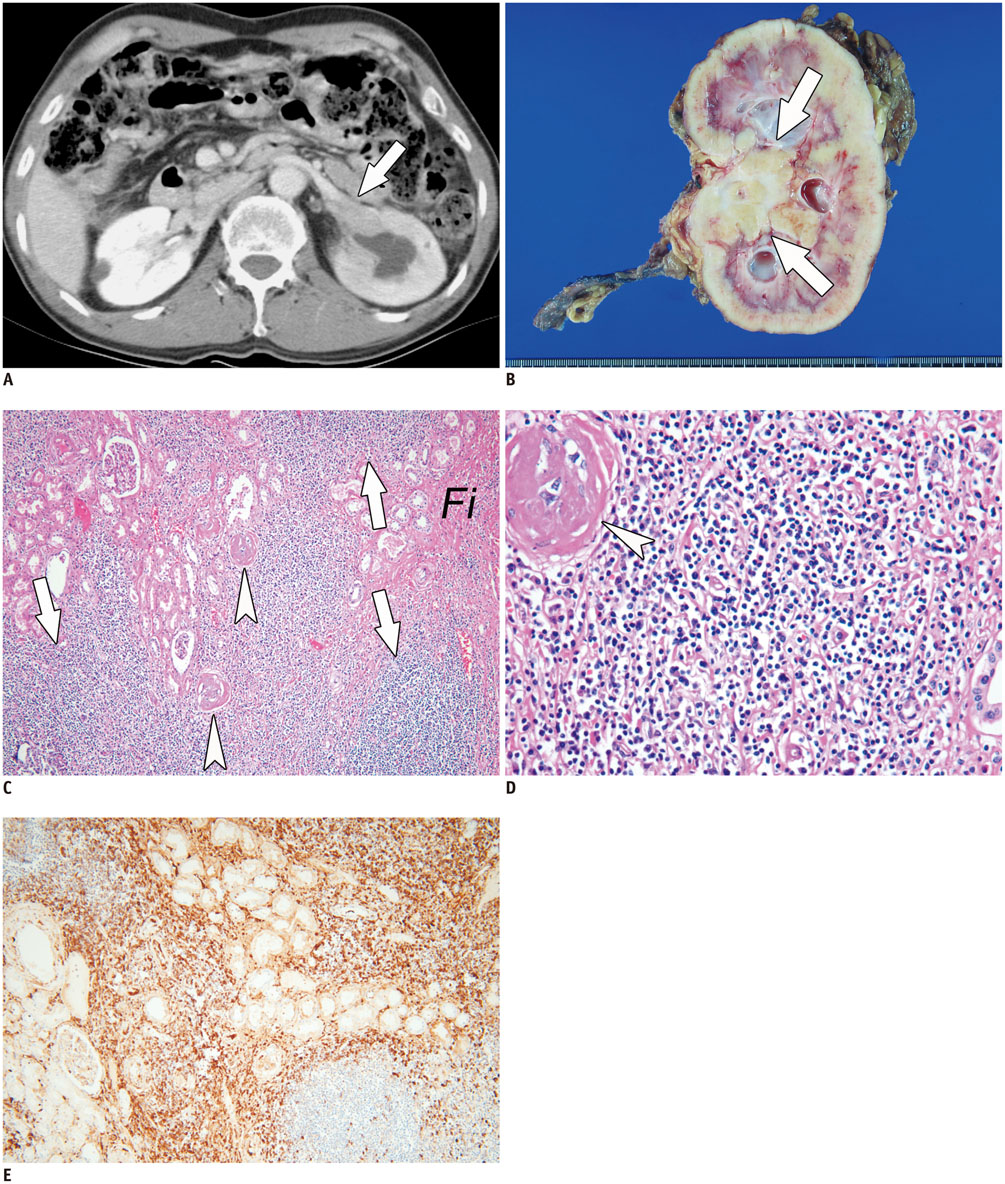
Fig. 1 72-year-old man who underwent left nephrectomy due to IgG4-KD mimicking urothelial carcinoma. A. Contrast-enhanced CT image shows ill-defined, homogeneous, soft-tissue mass (arrow) which encases left renal pelvis causing hydronephrosis. B. He underwent left nephrectomy with diagnosis of having urothelial carcinoma. Photograph of surgical specimen demonstrates lobulated, yellowish, firm mass (arrows) around renal pelvis. C, D. Lower-power (× 100) (C) and higher-power (× 400) (D) photomicrographs of histological specimen (hematoxylin and eosin staining) show dense plasma cell infiltration (arrows) with fibrous background (Fi) and obliterative phlebitis (arrowheads). E. IgG4 immunostaining (× 100) of histologic specimen shows numerous, brown, IgG4-positive plasma cells. IgG4-KD = immunoglobulin G4-related kidney disease
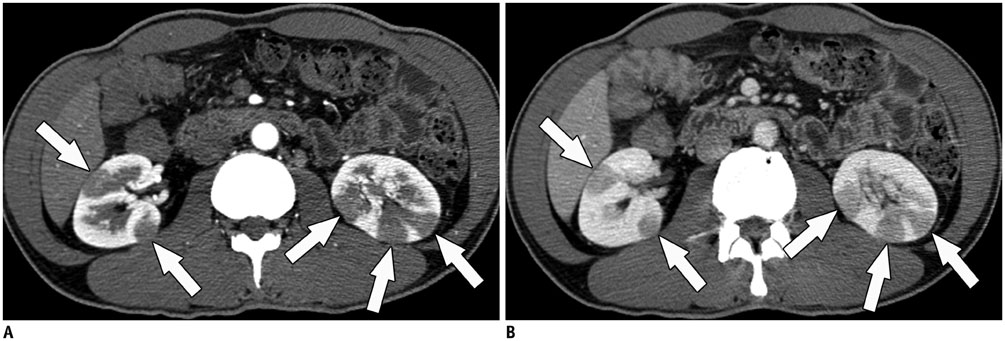
Fig. 2 49-year-old man with IgG4-KD manifesting as multiple, renal parenchymal nodules. A, B. Contrast-enhanced arterial (A) and portal (B) phase CT images show multiple, small, round or wedge-shaped, hypodense nodules (arrows) in both kidneys, predominantly in cortex. Renal nodules progressively enhance in portal phase. IgG4-KD = immunoglobulin G4-related kidney disease
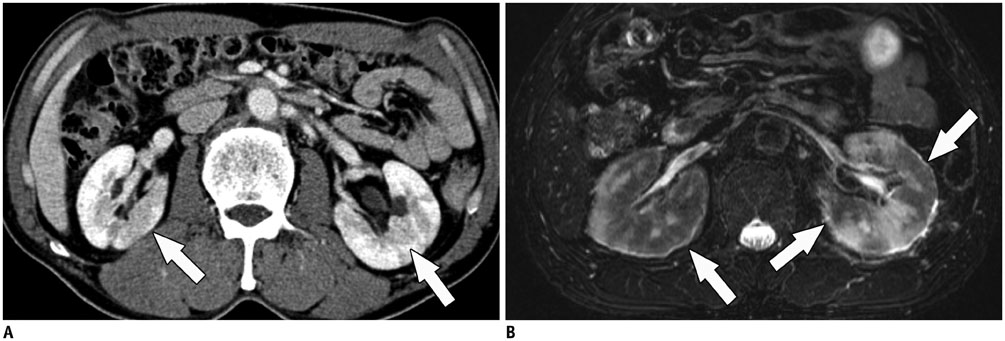
Fig. 3 IgG4-KD manifesting as diffuse patchy infiltrative parenchymal lesions. A. 66-year-old man. Contrast-enhanced portal phase CT image shows patchy infiltrative hypodense lesions (arrows) in both kidneys. B. 56-year-old man. T2-weighted MR image shows diffuse patchy infiltrative lesions appearing noticeably hypointense (arrows) in both kidneys. IgG4-KD = immunoglobulin G4-related kidney disease
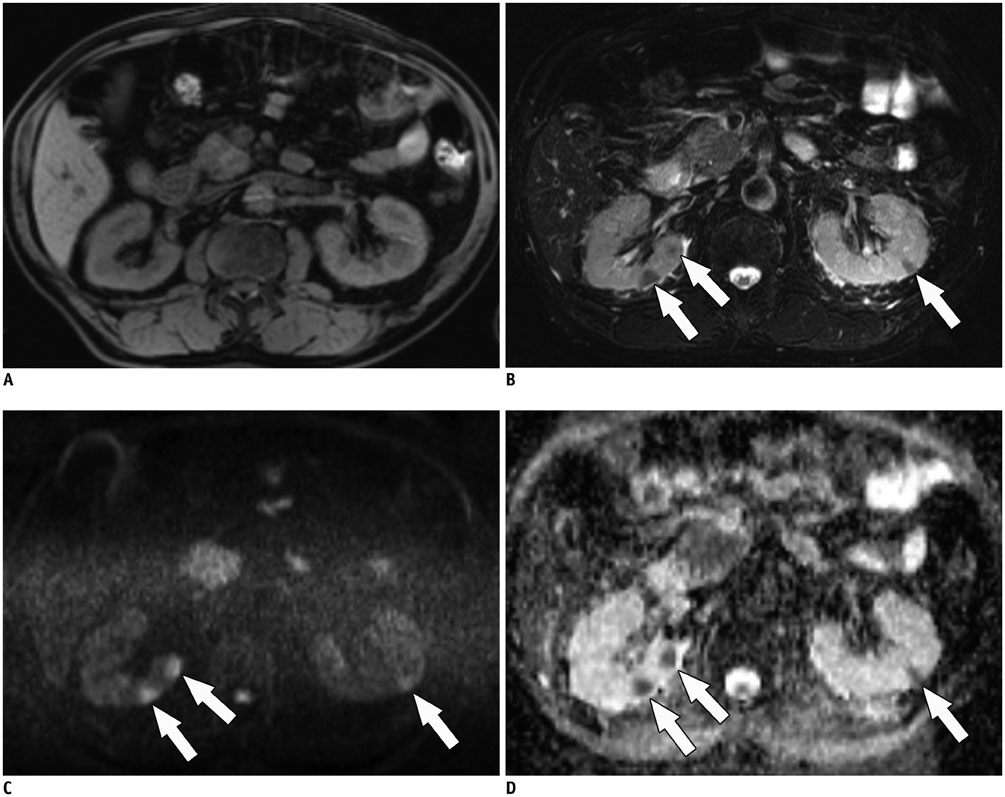
Fig. 4 MR imaging features of IgG4-KD in 64-year-old man. A. On precontrast T1-weighted image, isointense renal lesions are not perceptible. B. T2-weighted image shows three, small, hypointense cortical nodules (arrows) in both kidneys. C, D. DWI (b value, 1000 s/mm2) (C) and ADC map (D) reveal renal nodules (arrows) which appear as having obvious hyperintensity and hypointensity, respectively, and representing diffusion restriction. ADC = apparent diffusion coefficient, DWI = diffusion-weighted MR imaging, IgG4-KD = immunoglobulin G4-related kidney disease

Fig. 5 MR imaging features of IgG4-KD in 72-year-old man. A-C. Dynamic contrast-enhanced MR images show small cortical nodule (arrows) in right kidney, and which appears hypointense in arterial phase (A) and progressively enhanced in portal (B) and delayed (C) phases, gradually becoming indistinct as phase passes. D. On DWI (b value, 1000 s/mm2), right renal lesion exhibits striking hyperintensity (arrow). DWI = diffusion-weighted MR imaging, IgG4-KD = immunoglobulin G4-related kidney disease

Fig. 6 64-year-old man with IgG4-KD manifesting as unilateral renal pelvic lesion. Contrast-enhanced arterial phase CT image shows ill-defined, mildly enhancing, soft-tissue mass (arrow) encasing right renal pelvis and without hydronephrosis. IgG4-KD = immunoglobulin G4-related kidney disease
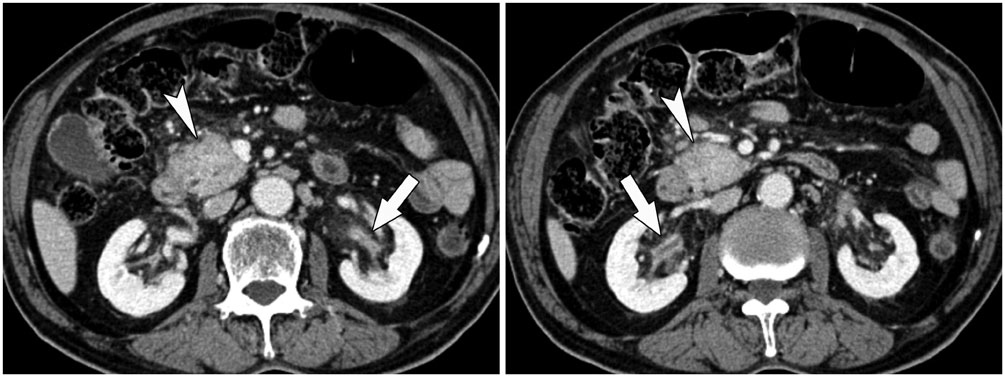
Fig. 7 84-year-old man with IgG4-KD manifesting as bilateral renal pelvic lesions. Contrast-enhanced portal phase CT images show mildly enhanced wall thickening of both renal pelvises (arrows) and without hydronephrosis. Pancreatic head enlargement with heterogeneous attenuation (arrowheads), indicating autoimmune pancreatitis, is also seen. IgG4-KD = immunoglobulin G4-related kidney disease
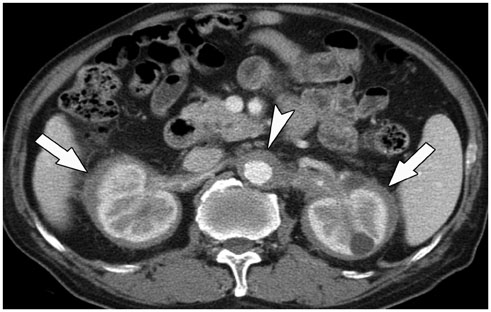
Fig. 8 74-year-old man with IgG4-KD manifesting as perinephric lesion. Contrast-enhanced arterial phase CT image shows homogeneous, rim-like, soft-tissue mass surrounding both kidneys (arrows). Peri-aortic, soft-tissue lesion, indicating retroperitoneal fibrosis, is also observed (arrowhead). IgG4-KD = immunoglobulin G4-related kidney disease
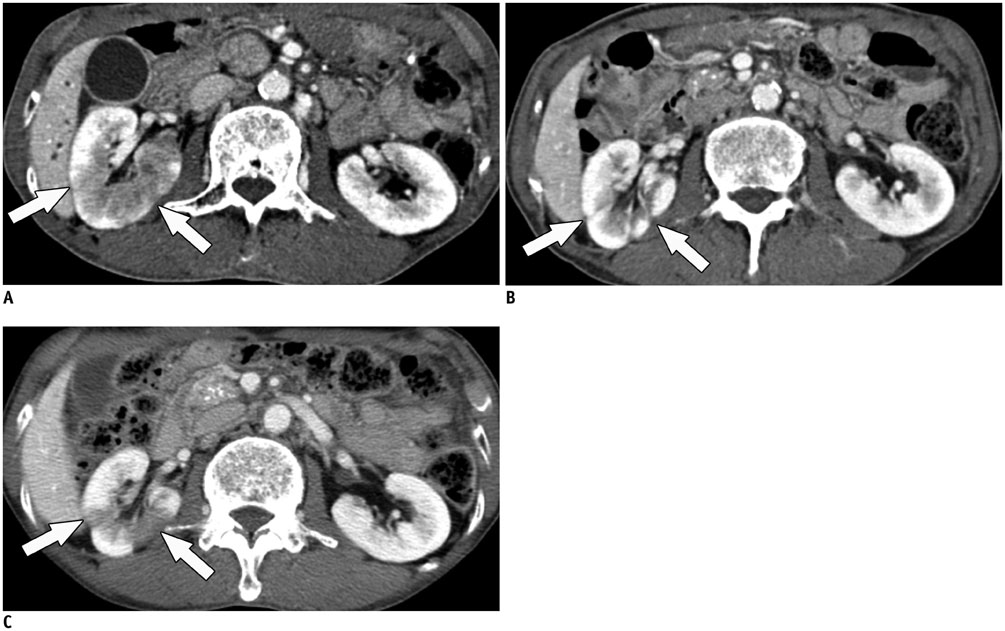
Fig. 9 Response of IgG4-KD to steroid therapy in 72-year-old man. A. Contrast-enhanced CT image shows diffuse infiltrative lesion (arrows) in right kidney. B. Contrast-enhanced CT image obtained after completion of steroid treatment demonstrates improvement of right renal lesion. However, multifocal, tiny cortical scars remain (arrows). C. Contrast-enhanced CT image obtained two years after steroid cessation reveals nodular or infiltrative lesions in right kidney (arrows), thus indicative of disease relapse. IgG4-KD = immunoglobulin G4-related kidney disease

Fig. 10 Mimickers of IgG4-KD manifesting as multiple, renal parenchymal lesions. A. 32-year-old woman with acute pyelonephritis. Contrast-enhanced delayed phase CT image shows multifocal, ill-defined, round and wedge-shaped, hypodense lesions (arrows) with mild swelling in left kidney. B. 53-year-old man with renal infarction. Contrast-enhanced arterial phase CT image shows large, rather well-demarcated, wedge-shaped areas of poor contrast enhancement (arrows) in both kidneys. C. 75-year-old man with renal metastases from lung cancer. Contrast-enhanced arterial phase CT image shows round, hypodense nodules (arrows) in both kidneys. D. 61-year-old man with renal lymphomas. Contrast-enhanced portal phase coronal CT image shows several, well-defined, homogeneous, round nodules/masses (arrows) in both kidneys. IgG4-KD = immunoglobulin G4-related kidney disease
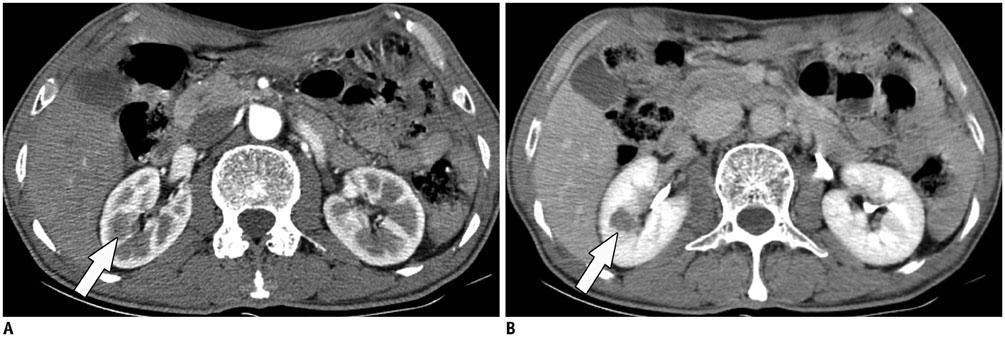
Fig. 11 Mimicker of IgG4-KD manifesting as single parenchymal nodule. A, B. 78-year-old man with chromophobe-type renal cell carcinoma. Contrast-enhanced arterial (A) and delayed (B) phase CT images demonstrate single hypovascular nodule (arrows) in right kidney. IgG4-KD = immunoglobulin G4-related kidney disease
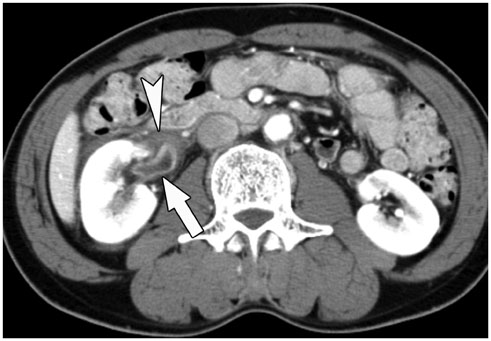
Fig. 12 Mimicker of IgG4-KD manifesting as renal pelvic lesion. 63-year-old man with transitional cell carcinoma. Contrast-enhanced portal phase CT image shows diffusely enhancing wall thickening of right renal pelvis (arrow) and surrounding soft-tissue lesion (arrowhead). IgG4-KD = immunoglobulin G4-related kidney disease
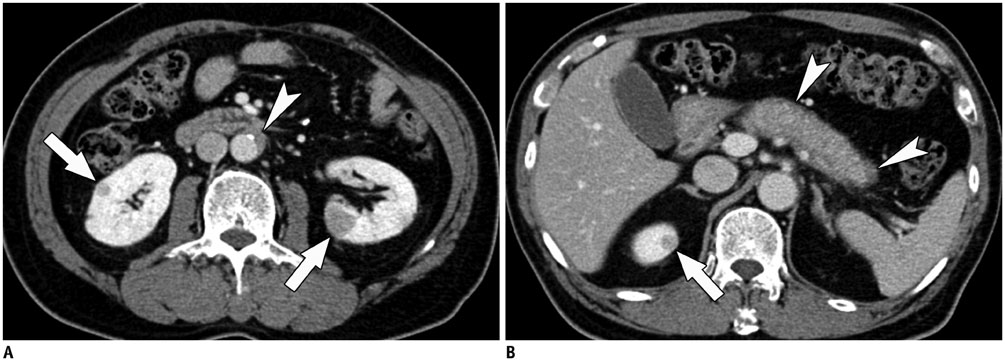
Fig. 13 Retroperitoneal fibrosis and autoimmune pancreatitis as clues to diagnosis of IgG4-KD in 71-year-old man. A, B. Contrast-enhanced portal phase CT images show several, well-defined, round, hypodense nodules (arrows) in both kidneys. Differential diagnosis for these renal lesions would be lymphoma, metastasis or IgG4-KD. However, periaortic, soft-tissue lesion (arrowhead in A) suggesting retroperitoneal fibrosis and sausage-shaped pancreas swelling with peripancreatic hypodense rim (arrowheads in B) which is typical of AIP, are observed together. Accordingly, such renal lesions can confidently be diagnosed as IgG4-KD. AIP = autoimmune pancreatitis, IgG4-KD = immunoglobulin G4-related kidney disease
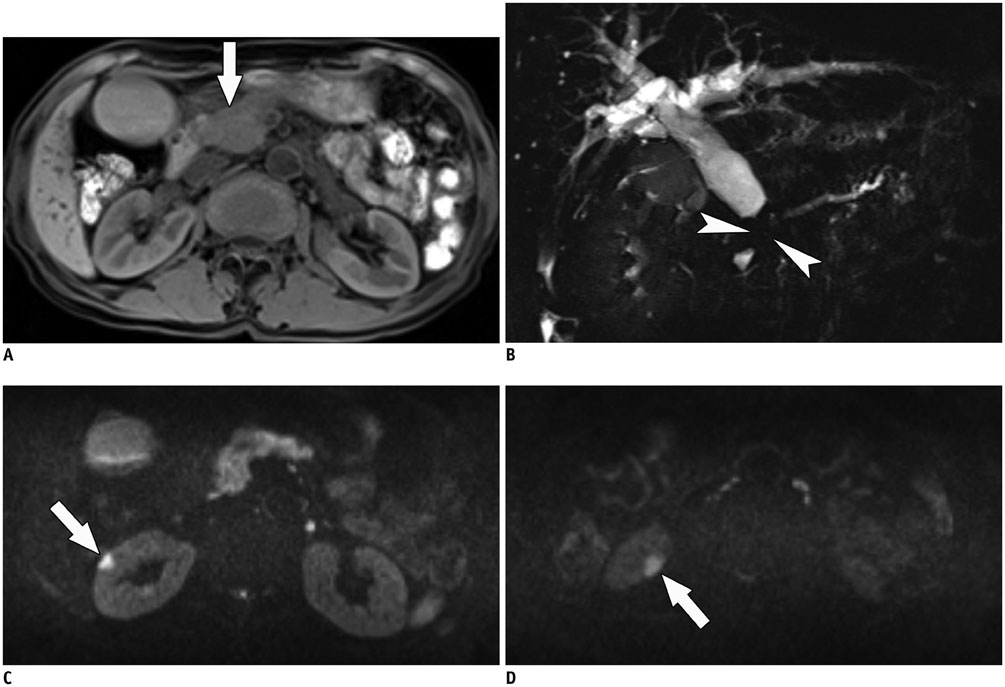
Fig. 14 IgG4-KD as clue for differentiating autoimmune pancreatitis from pancreatic cancer in 64-year-old man. A, B. Precontrast T1-weighted MR image (A) shows hypointense, mass-like enlargement of pancreatic head (arrow). MR cholangiopancreatography (B) shows abrupt, severe narrowing of pancreatic and bile ducts (arrowheads) with upstream duct dilatation. These MR findings are highly suggestive of pancreatic cancer. C, D. DWIs (b value, 1000 s/mm2) show multifocal, hyperintense nodules (arrows) in right kidney. Combination of these renal lesions and pancreatic mass/enlargement strongly suggests IgG4-SD, i.e., IgG4-KD and focal type AIP. AIP = autoimmune pancreatitis, DWI = diffusion-weighted MR imaging, IgG4-KD = immunoglobulin G4-related kidney disease, IgG4-SD = IgG4-related sclerosing disease
Reference
-
1. Cornell LD. IgG4-related kidney disease. Semin Diagn Pathol. 2012; 29:245–250.2. Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012; 366:539–551.3. Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012; 25:1181–1192.4. Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012; 22:21–30.5. Raissian Y, Nasr SH, Larsen CP, Colvin RB, Smyrk TC, Takahashi N, et al. Diagnosis of IgG4-related tubulointerstitial nephritis. J Am Soc Nephrol. 2011; 22:1343–1352.6. Saeki T, Kawano M, Mizushima I, Yamamoto M, Wada Y, Nakashima H, et al. The clinical course of patients with IgG4-related kidney disease. Kidney Int. 2013; 84:826–833.7. Kawano M, Saeki T, Nakashima H, Nishi S, Yamaguchi Y, Hisano S, et al. Proposal for diagnostic criteria for IgG4-related kidney disease. Clin Exp Nephrol. 2011; 15:615–626.8. Khalili K, Doyle DJ, Chawla TP, Hanbidge AE. Renal cortical lesions in patients with autoimmune pancreatitis: a clue to differentiation from pancreatic malignancy. Eur J Radiol. 2008; 67:329–335.9. Kim B, Kim JH, Byun JH, Kim HJ, Lee SS, Kim SY, et al. IgG4-related kidney disease: MRI findings with emphasis on the usefulness of diffusion-weighted imaging. Eur J Radiol. 2014; 83:1057–1062.10. Saeki T, Nishi S, Imai N, Ito T, Yamazaki H, Kawano M, et al. Clinicopathological characteristics of patients with IgG4-related tubulointerstitial nephritis. Kidney Int. 2010; 78:1016–1023.11. Khosroshahi A, Stone JH. A clinical overview of IgG4-related systemic disease. Curr Opin Rheumatol. 2011; 23:57–66.12. Takahashi N, Kawashima A, Fletcher JG, Chari ST. Renal involvement in patients with autoimmune pancreatitis: CT and MR imaging findings. Radiology. 2007; 242:791–801.13. Kim JH, Kim MH, Byun JH, Lee SS, Lee SJ, Park SH, et al. Diagnostic strategy for differentiating autoimmune pancreatitis from pancreatic cancer: is an endoscopic retrograde pancreatography essential. Pancreas. 2012; 41:639–647.14. Kuroda N, Nakamura S, Miyazaki K, Inoue K, Ohara M, Mizuno K, et al. Chronic sclerosing pyelitis with an increased number of IgG4-positive plasma cells. Med Mol Morphol. 2009; 42:236–238.15. Kim SA, Lee SR, Huh J, Shen SS, Ro JY. IgG4-associated inflammatory pseudotumor of ureter: clinicopathologic and immunohistochemical study of 3 cases. Hum Pathol. 2011; 42:1178–1184.16. Sharma SG, Vlase HL, D'Agati VD. IgG4-related tubulointerstitial nephritis with plasma cell-rich renal arteritis. Am J Kidney Dis. 2013; 61:638–643.17. Saeki T, Kawano M. IgG4-related kidney disease. Kidney Int. 2014; 85:251–257.18. Yamaguchi Y, Kanetsuna Y, Honda K, Yamanaka N, Kawano M, Nagata M. Japanese study group on IgG4-related nephropathy. Characteristic tubulointerstitial nephritis in IgG4-related disease. Hum Pathol. 2012; 43:536–549.19. Triantopoulou C, Malachias G, Maniatis P, Anastopoulos J, Siafas I, Papailiou J. Renal lesions associated with autoimmune pancreatitis: CT findings. Acta Radiol. 2010; 51:702–707.20. Hedgire SS, McDermott S, Borczuk D, Elmi A, Saini S, Harisinghani MG. The spectrum of IgG4-related disease in the abdomen and pelvis. AJR Am J Roentgenol. 2013; 201:14–22.21. Vlachou PA, Khalili K, Jang HJ, Fischer S, Hirschfield GM, Kim TK. IgG4-related sclerosing disease: autoimmune pancreatitis and extrapancreatic manifestations. Radiographics. 2011; 31:1379–1402.22. Manfredi R, Frulloni L, Mantovani W, Bonatti M, Graziani R, Pozzi Mucelli R. Autoimmune pancreatitis: pancreatic and extrapancreatic MR imaging-MR cholangiopancreatography findings at diagnosis, after steroid therapy, and at recurrence. Radiology. 2011; 260:428–436.23. Pozdzik AA, Matos C, Rorive S, Brocheriou I, Delhaye M, Nortier JL. Diffusion-weighted magnetic resonance imaging: a non-nephrotoxic prompt assessment of kidney involvement in IgG4-related disease. Kidney Int. 2014; 85:981.24. Sasiwimonphan K, Gorman B, Kawashima A, Chari ST, Takahashi N. Renal involvement in patients with autoimmune pancreatitis: ultrasound findings. Eur J Radiol. 2012; 81:807–810.25. Saunders HS, Dyer RB, Shifrin RY, Scharling ES, Bechtold RE, Zagoria RJ. The CT nephrogram: implications for evaluation of urinary tract disease. Radiographics. 1995; 15:1069–1085. discussion 1086-108826. Kawashima A, Sandler CM, Goldman SM, Raval BK, Fishman EK. CT of renal inflammatory disease. Radiographics. 1997; 17:851–866. discussion 867-86827. Suzer O, Shirkhoda A, Jafri SZ, Madrazo BL, Bis KG, Mastromatteo JF. CT features of renal infarction. Eur J Radiol. 2002; 44:59–64.28. Wong WS, Moss AA, Federle MP, Cochran ST, London SS. Renal infarction: CT diagnosis and correlation between CT findings and etiologies. Radiology. 1984; 150:201–205.29. Honda H, Coffman CE, Berbaum KS, Barloon TJ, Masuda K. CT analysis of metastatic neoplasms of the kidney. Comparison with primary renal cell carcinoma. Acta Radiol. 1992; 33:39–44.30. Bracken RB, Chica G, Johnson DE, Luna M. Secondary renal neoplasms: an autopsy study. South Med J. 1979; 72:806–807.31. Ganeshan D, Iyer R, Devine C, Bhosale P, Paulson E. Imaging of primary and secondary renal lymphoma. AJR Am J Roentgenol. 2013; 201:W712–W719.32. Jafri SZ, Bree RL, Amendola MA, Glazer GM, Schwab RE, Francis IR, et al. CT of renal and perirenal non-Hodgkin lymphoma. AJR Am J Roentgenol. 1982; 138:1101–1105.33. Semelka RC, Kelekis NL, Burdeny DA, Mitchell DG, Brown JJ, Siegelman ES. Renal lymphoma: demonstration by MR imaging. AJR Am J Roentgenol. 1996; 166:823–827.34. Saremi F, Knoll AN, Bendavid OJ, Schultze-Haakh H, Narula N, Sarlati F. Characterization of genitourinary lesions with diffusion-weighted imaging. Radiographics. 2009; 29:1295–1317.35. Yamashita Y, Takahashi M, Watanabe O, Yoshimatsu S, Ueno S, Ishimaru S, et al. Small renal cell carcinoma: pathologic and radiologic correlation. Radiology. 1992; 184:493–498.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Systemic Manifestations of Immunoglobulin G4-Related Disease: A Pictorial Essay
- Overview of the Immunoglobulin G4-related Disease Spectrum
- Immunoglobulin G4-Related Systemic Sclerosing Disease: A Case Involving the Ureter and Kidney
- Immunoglobulin G4-Related Disease Involving Various Head and Neck Regions: A Case Report
- Immunoglobulin G4-related sclerosing cholangitis
