Korean J Gastroenterol.
2014 Sep;64(3):164-167. 10.4166/kjg.2014.64.3.164.
Two Cases of Electrocautery Incision Therapy Using an Insulated-tip Knife for Treatment of Symptomatic Benign Short-segment Colonic Stenosis Following Colonic Resection
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea. hankoonhee@hanmail.net
- KMID: 2160659
- DOI: http://doi.org/10.4166/kjg.2014.64.3.164
Abstract
- Anastomotic stenosis of the colon is not an uncommon finding; however, its frequency varies from one study to another. Traditionally, postoperative colonic stenosis is managed surgically. However, endoscopic therapy has recently become the preferred treatment modality over traditional surgery. Good short-term success has been achieved with use of endoscopic balloon dilation; however, restenosis may occur over time in 14% to 25% of patients. The current report showed the effectiveness and usefulness of an insulated-tip knife (IT-knife) for electrocautery therapy of a patient with symptomatic anastomotic colonic stenosis.
Keyword
MeSH Terms
Figure
-

Fig. 1. Case 1: Endoscopic appearance of colorectal stenosis.
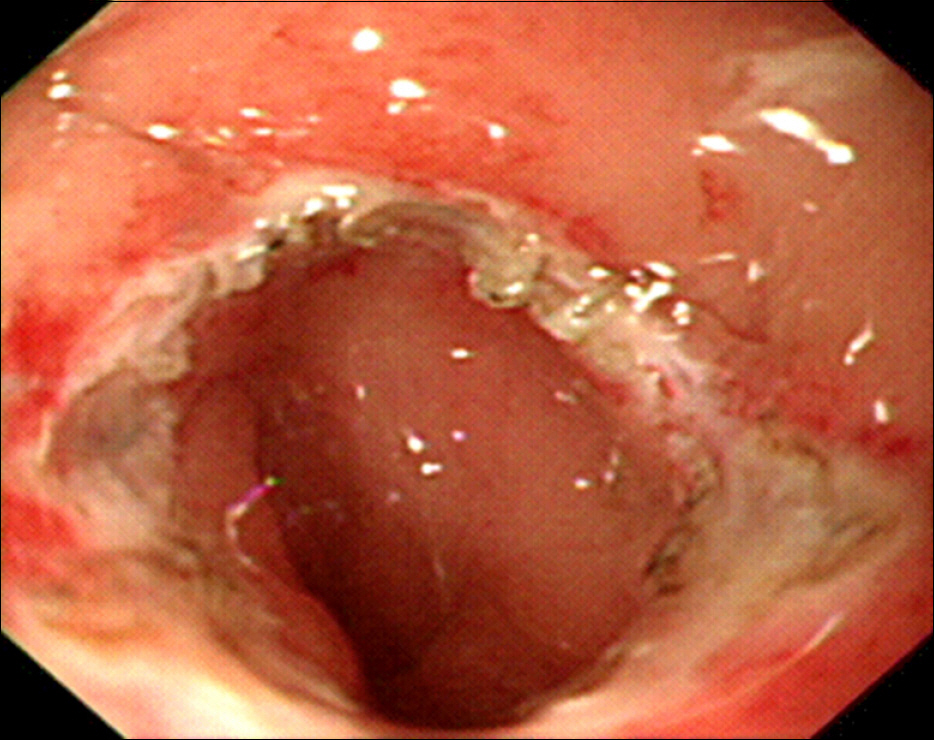
Fig. 2. Case 1: Radial incision of the stenosis using an insulated-tip knife.

Fig. 3. Case 1: An endoscopic finding at 12 months after dilatation.
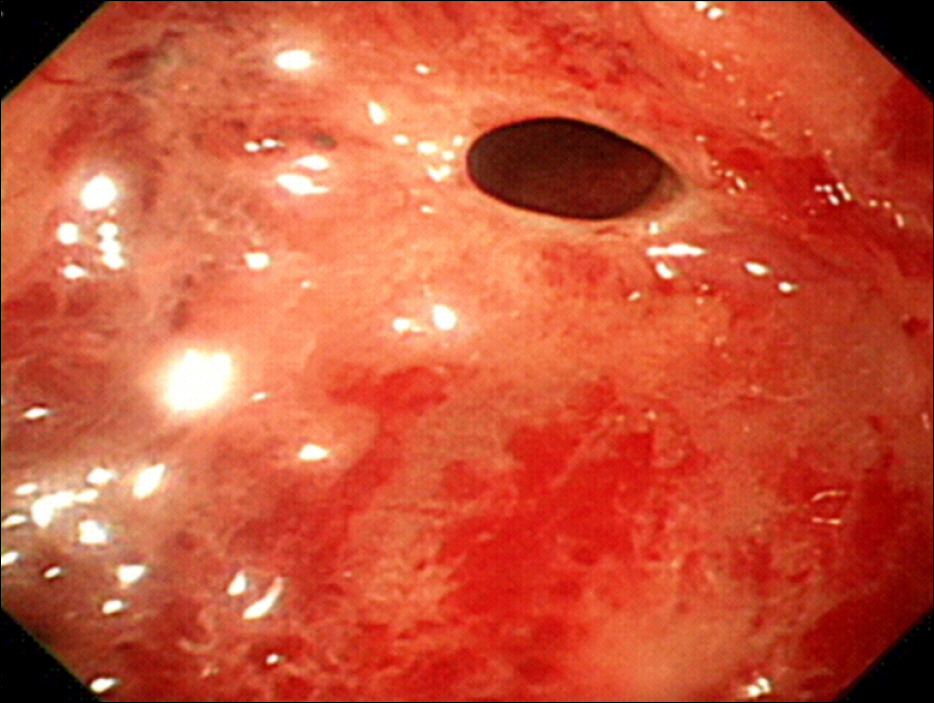
Fig. 4. Case 2: Endoscopic appearance of colorectal stenosis.

Fig. 5. Case 2: Radial incision of the stenosis using an insulated-tip knife.
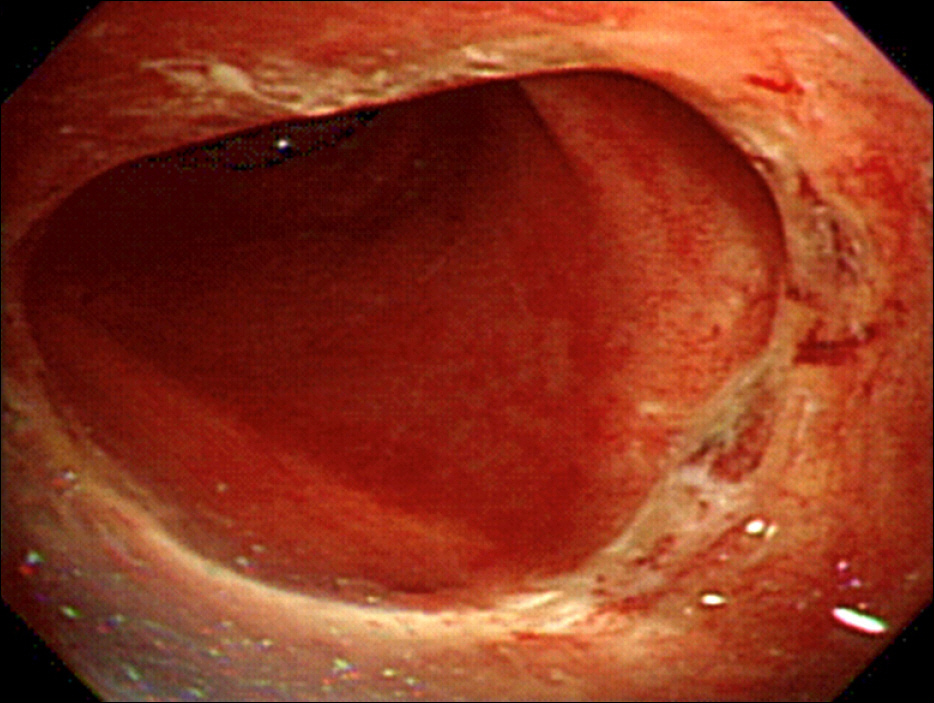
Fig. 6. Case 2: An endoscopic finding at seven months after dilatation.
Reference
-
References
1. Lew RJ, Kochman ML. A review of endoscopic methods of esophageal dilation. J Clin Gastroenterol. 2002; 35:117–126.
Article2. Grossman EB, Schattner MA, Dimaio CJ, Gerdes H, Wong DW, Markowitz AJ. Endoscopic management of complete colonic obstruction. J Interv Gastroenterol. 2011; 1:179–181.
Article3. Solt J, Bajor J, Szabó M, Horváth OP. Long-term results of balloon catheter dilation for benign gastric outlet stenosis. Endoscopy. 2003; 35:490–495.
Article4. Kerkhof M, Dewint P, Koch AD, van der Woude CJ. Endoscopic needle-knife treatment of refractory ileo-ascending anastomotic stricture. Endoscopy. 2013; 45(Suppl 2):E57–E58.
Article5. Brandimarte G, Tursi A, Gasbarrini G. Endoscopic treatment of benign anastomotic colorectal stenosis with electrocautery. Endoscopy. 2000; 32:461–463.
Article6. de Lange EE, Shaffer HA Jr. Rectal strictures: treatment with fluo-roscopically guided balloon dilation. Radiology. 1991; 178:475–479.
Article7. Weinstock LB, Shatz BA. Endoscopic abnormalities of the anastomosis following resection of colonic neoplasm. Gastrointest Endosc. 1994; 40:558–561.
Article8. Kozarek RA. Hydrostatic balloon dilation of gastrointestinal stenoses: a national survey. Gastrointest Endosc. 1986; 32:15–19.
Article9. Truong S, Willis S, Schumpelick V. Endoscopic therapy of benign anastomotic strictures of the colorectum by electroincision and balloon dilatation. Endoscopy. 1997; 29:845–849.
Article10. Virgilio C, Cosentino S, Favara C, Russo V, Russo A. Endoscopic treatment of postoperative colonic strictures using an achalasia dilator: short-term and long-term results. Endoscopy. 1995; 27:219–222.
Article11. Park CH, Kim JI, Oh ST, Lee MD, Kim SK, Kim IC. Endoscopic balloon dilatation for benign anastomotic stricture following esophageal resection. Korean J Gastroenterol. 1997; 30:294–302.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- High grade anorectal stricture complicating Crohn's disease: endoscopic treatment using insulated-tip knife
- Endoscopic Incision Therapy by Needle Knife Papillotome in the Treatment of Postoperative Anastomotic Stenosis
- An Intractable Caustic Esophageal Stricture Successfully Managed with Sequential Treatment Comprising Incision with an Insulated-Tip Knife, Balloon Dilation, and an Oral Steroid
- Endoscopic Mucosal Resection Using Insulated-tip Electrosurgical Knife
- Successful Endoscopic Resection of Residual Colonic Mucosa-Associated Lymphoid Tissue Lymphoma after Polypectomy
