Papillary Thyroid Carcinoma with Retropharyngeal Node Metastasis Demonstrating Negative I-131 but Positive FDG Uptake on PET/CT
- Affiliations
-
- 1Department of Surgery, Catholic Kwandong University International St. Mary's Hospital, Catholic Kwandong University College of Medicine, Incheon, Korea. iklee@ish.ac.kr
- 2Department of Surgery, Graduate School, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Otorhinolaryngology-Head and Neck Surgery, Catholic Kwandong University International St. Mary's Hospital, Catholic Kwandong University College of Medicine, Incheon, Korea.
- 4Department of Nuclear Medicine, Catholic Kwandong University International St. Mary's Hospital, Catholic Kwandong University College of Medicine, Incheon, Korea.
- 5Department of Radiology, Catholic Kwandong University International St. Mary's Hospital, Catholic Kwandong University College of Medicine, Incheon, Korea.
- KMID: 2158624
- DOI: http://doi.org/10.16956/kaes.2016.16.1.18
Abstract
- Papillary thyroid carcinoma (PTC) is commonly accompanied by cervical lymph node metastasis, whereas metastases to the retropharyngeal lymph nodes (RPN) are rare. Radioactive iodine (RAI) ablation is recommended for detection and treatment of differentiated thyroid carcinoma (DTC). However, in some cases of iodine-negative DTC, F-18 fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) can aid in detection of additional lesions. We report on a patient with PTC who had retropharyngeal node involvement with iodine-negative features and low thyroglobulin level at the time of diagnosis but with metastasis identified on FDG PET/CT.
MeSH Terms
Figure
-
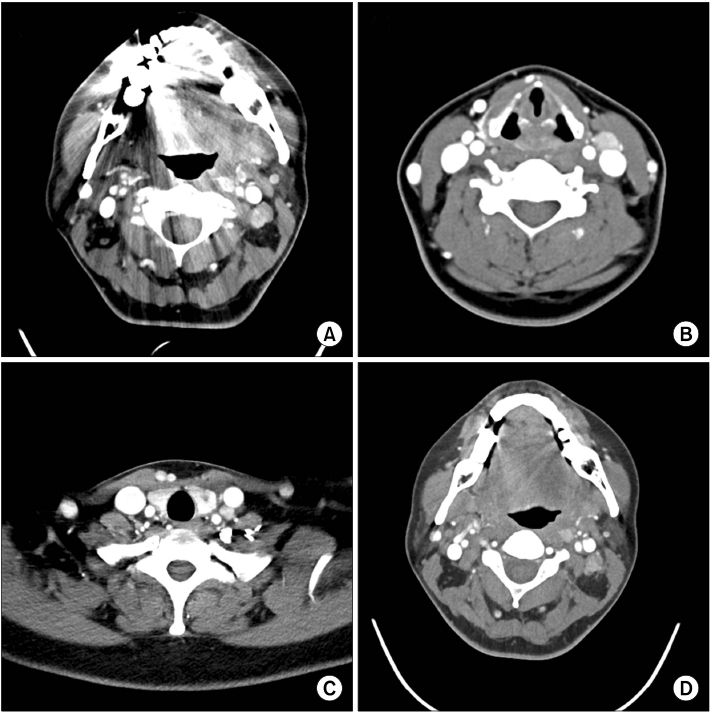
Fig. 1 Images of preoperative CT showing multiple neck lymph node metastases. Contrast-enhanced CT images showing multiple hyper-enhancing lymph nodes in the left retropharyngeal space and left neck at level 2 (A), level 3 (B), and level 4 (C). On contrast-enhanced CT images obtained one year after surgery, enlarged, enhancing lymph nodes remain in the left retropharyngeal space and left neck level 2 (D). The sizes of the residual contrast-enhancing lymph nodes did not significantly change during the follow-up period.
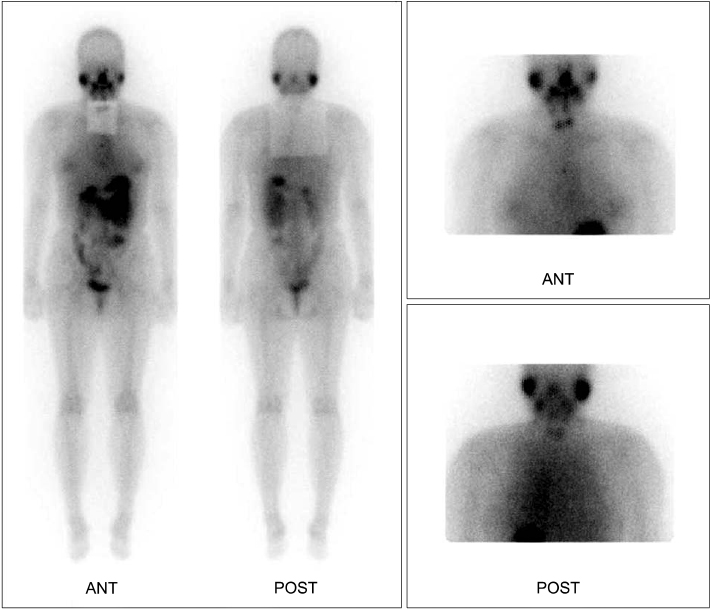
Fig. 2 Anterior and posterior images of the post-ablative I-131 scan. Three months after total thyroidectomy, the patient underwent I-131 ablation with a dose of 5.55 GBq. Post-ablative scanning performed three days after I-131 administration shows a focus of increased I-131 uptake in the thyroid bed, suggesting remnant thyroid uptake. With the exception of remnant thyroid uptake, no other abnormal I-131 uptake suggesting thyroid cancer metastasis is seen.
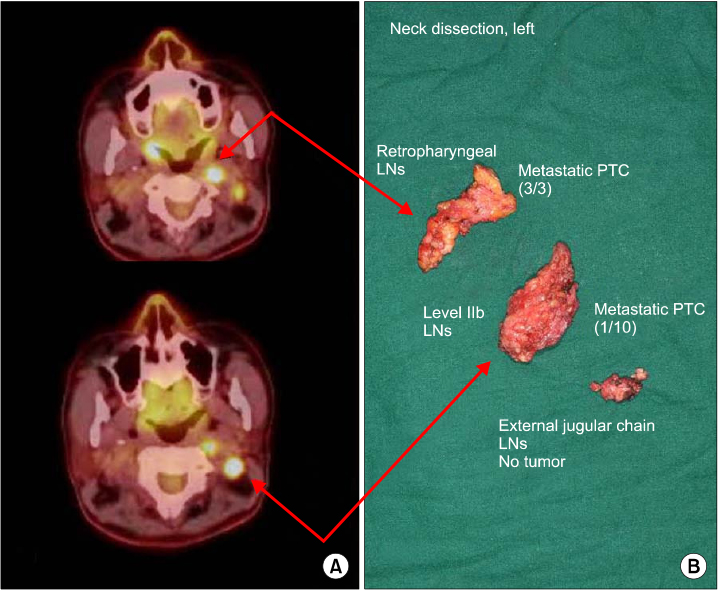
Fig. 3 (A) Two enlarged lymph nodes with increased FDG uptake were noted in the left neck level II (SUVmax of 11.1) and retropharyngeal space (SUVmax of 17.6) on fused trans-axial FDG PET/CT images. (B) Retropharyngeal and level IIb lymph node involvement was verified as metastatic papillary thyroid carcinoma.
Reference
-
1. Togashi T, Sugitani I, Toda K, Kawabata K, Takahashi S. Surgical management of retropharyngeal nodes metastases from papillary thyroid carcinoma. World J Surg. 2014; 38:2831–2837.
Article2. Lee JW, Lee SM, Lee DH, Kim YJ. Clinical utility of 18F-FDG PET/CT concurrent with 131I therapy in intermediateto-high-risk patients with differentiated thyroid cancer: dual-center experience with 286 patients. J Nucl Med. 2013; 54:1230–1236.
Article3. Mirallié E, Guillan T, Bridji B, Resche I, Rousseau C, Ansquer C, et al. Therapeutic impact of 18FDG-PET/CT in the management of iodine-negative recurrence of differentiated thyroid carcinoma. Surgery. 2007; 142:952–958.
Article4. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009; 19:1167–1214.
Article5. Lee J, Sung TY, Nam KH, Chung WY, Soh EY, Park CS. Is level IIb lymph node dissection always necessary in N1b papillary thyroid carcinoma patients. World J Surg. 2008; 32:716–721.
Article6. Merdad M, Eskander A, Kroeker T, Freeman JL. Metastatic papillary thyroid cancer with lateral neck disease: pattern of spread by level. Head Neck. 2013; 35:1439–1442.
Article7. Cheng PT, Hao SP, Lin YH, Yeh AR. Objective comparison of shoulder dysfunction after three neck dissection techniques. Ann Otol Rhinol Laryngol. 2000; 109:761–766.
Article8. Lee CR, Nam KH. Lateral neck node dissection in differentiated thyroid carcinoma. Korean J Endocr Surg. 2014; 14:1–6.
Article9. Leger AF, Baillet G, Dagousset F, Vincenot MI, Izembart M, Clerc J, et al. Upper retropharyngeal node involvement in differentiated thyroid carcinoma demonstrated by 131I scintigraphy. Br J Radiol. 2000; 73:1260–1264.
Article10. Rouvière H. Anatomy of the human lymphatic system. Ann Arbor: Edwards Brothers;1938. p. 5–65.11. Kim WG, Yoon JH, Kim WB, Kim TY, Kim EY, Kim JM, et al. Change of serum antithyroglobulin antibody levels is useful for prediction of clinical recurrence in thyroglobulin-negative patients with differentiated thyroid carcinoma. J Clin Endocrinol Metab. 2008; 93:4683–4689.
Article12. Park EK, Chung JK, Lim IH, Park do J, Lee DS, Lee MC, et al. Recurrent/metastatic thyroid carcinomas false negative for serum thyroglobulin but positive by posttherapy I-131 whole body scans. Eur J Nucl Med Mol Imaging. 2009; 36:172–179.
Article13. Bachelot A, Cailleux AF, Klain M, Baudin E, Ricard M, Bellon N, et al. Relationship between tumor burden and serum thyroglobulin level in patients with papillary and follicular thyroid carcinoma. Thyroid. 2002; 12:707–711.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Transoral Resection of Retropharyngeal Lymph Node Metastasis from Papillary Thyroid Carcinoma Diagnosed by PET-CT Follow-Up after Lateral Neck Dissection
- Comparison of Neck CT and ¹â¸F-FDG PET-CT for Making the Preoperative Diagnosis of Lymph Node Metastasis in Papillary Thyroid Cancer
- FDG Uptake in the Pathologically Proven Papillary Thyroid Cancer
- Retropharyngeal Lymph Node Metastasis of Thyroid Papillary Carcinoma
- Retropharyngeal Lymph Node Metastasis from Thyroid Papillary Carcinoma with Airway Obstruction
