Recurrent Juvenile Nasopharyngeal Angiofibroma Treated with Gamma Knife Surgery
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University College of Medicine, Clinical Research Institute, Medical Research Center, Seoul National University Hospital, Seoul, Korea. gknife@plaza.snu.ac.kr
- KMID: 2157839
- DOI: http://doi.org/10.3346/jkms.2006.21.4.773
Abstract
- Radiosurgery has been rarely applied for juvenile nasopharyngeal angiofibroma (JNA) and cumulative reports are lacking. The authors report a case of successful treatment of recurred JNA with gamma knife surgery (GKS). A 48-yr-old man was presented with right visual acuity deterioration and brain magnetic resonance images (MRI) disclosed a 3 cm-sized intraorbital mass in the right orbit. He underwent a right fronto-temporal craniotomy and the mass was subtotally removed to preserve visual function. Histological diagnosis confirmed JNA in typical nature. However, the vision gradually worsened to fail four years after operation. MRI then showed regrowth of the tumor occupying most of the right orbit. GKS was done for the re-curred lesion. A dose of 17 Gy was delivered to the 50% isodose line of tumor mar-gin. During the following four-year follow-up period, the mass disappeared almost completely without any complications. Usually JNA can be exclusively diagnosed by radiological study alone. So this report of successful treatment of JNA with GKS may provide an important clue for the novel indication of GKS.
Keyword
MeSH Terms
Figure
-

Fig. 1 Preoperative axial Gd-DTPA-enhanced T1-weighted magnetic resonance image (A) demonstrating homogeneously enhancing mass in the right orbit. This mass was subtotally removed with small residual remaining in the orbital cone as postoperative computed tomography shows (B).
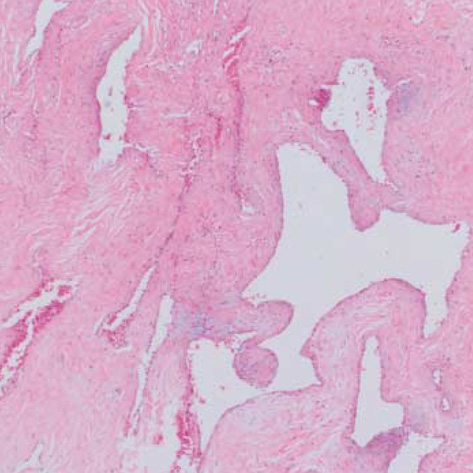
Fig. 2 Histopathological appearance of juvenile nasopharyngeal angiofibroma. Note typical feature of dense fibro-colllagenous tissue with interspersed slit-like and gaping vascular channels (H&E, ×45).
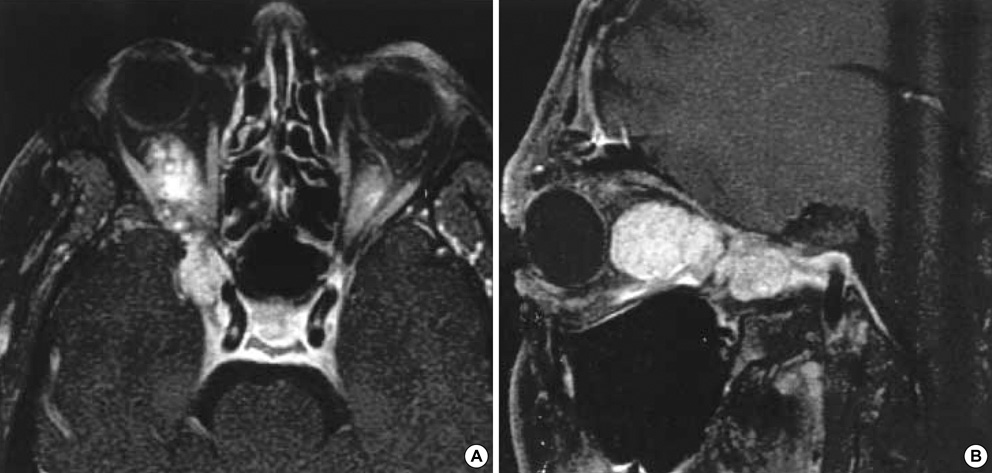
Fig. 3 Axial (A) and sagittal (B) Gd-DTPA-enhanced T1-weighted magnetic resonance images obtained four years after the initial surgery. Multilobulated homogeneously enhancing recurrent mass in the right orbit extending to the inferior orbital fissure and cavernous sinus is shown.
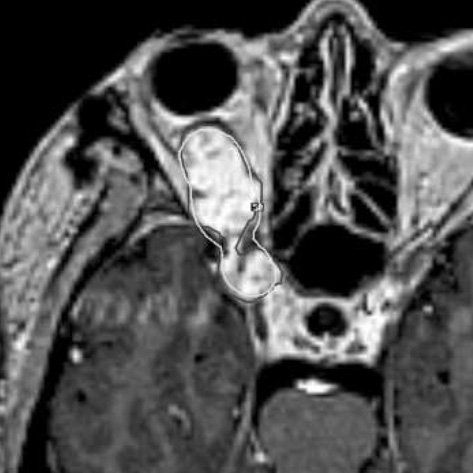
Fig. 4 Axial Gd-DTPA-enhanced T1-weighted magnetic resonance image showing dose distribution for gamma knife surgery. Total volume is measured 6.8 cm3. A dose of 17 Gy was delivered to the 50% isodose line of tumor margin.

Fig. 5 Serial follow-up Gd-DTPA-enhanced T1-weighted magnetic resonance images after gamma knife surgery. Gradual decrease in size of the mass is noted after a year with total volume of 2.2 cm3 (A) and two years with 0.97 cm3 (B), and finally disappeared four years after the gamma knife surgery (C).
Reference
-
1. Neel HB 3rd, Whicker JH, Devine KD, Weiland LH. Juvenile angiofibroma. Review of 120 cases. Am J Surg. 1973. 26:547–556.2. Gullane PJ, Davidson J, O'Dwyer T, Forte V. Juvenile angiofibroma:a review of the literature and a case series report. Laryngoscope. 1992. 102:928–933.3. Patterson CN. Juvenile nasopharyngeal angiofibroma. Otolaryngol Clin North Am. 1973. 6:839–861.
Article4. Cummings BJ, Blend R, Keane T, Fitzpatrick P, Beale F, Clark R, Garrett P, Harwood A, Payne D, Rider W. Primary radiation therapy for juvenile nasopharyngeal angiofibroma. Laryngoscope. 1984. 94:1599–1605.
Article5. Lee JT, Chen P, Safa A, Juillard G, Calcaterra TC. The role of radiation in the treatment of advanced juvenile angiofibroma. Laryngoscope. 2002. 112:1213–1220.
Article6. Scholtz AW, Appenroth E, Kammen-Jolly K, Scholtz LU, Thumfart WF. Juvenile nasopharyngeal angiofibroma: management and therapy. Laryngoscope. 2001. 111:681–687.
Article7. Jafek BW, Nahum AM, Butler RM, Ward PH. Surgical treatment of juvenile nasopharyngeal angiofibroma. Laryngoscope. 1973. 83:707–720.
Article8. Dei Tos AP, Seregard S, Calonje E, Chan JK, Fletcher CD. Giant cell angiofibroma. A distinctive orbital tumor in adults. Am J Surg Pathol. 1995. 19:1286–1293.9. Guillou L, Gebhard S, Coindre JM. Orbital and extraorbital giant cell angiofibroma: A giant cell-rich variant of solitary fibrous tumor? Clinicopathologic and immunohistochemical analysis of a series in favor of a unifying concept. Am J Surg Pathol. 2000. 24:971–979.10. Jafek BW, Krekorian EA, Kirsch WM, Wood RP. Juvenile nasopharyngeal angiofibroma: management of intracranial extension. Head Neck Surg. 1979. 2:119–128.
Article11. Jereb B, Anggard A, Baryd I. Juvenile nasopharyngeal angiofibroma: a clinical study of 69 cases. Acta Radiol Ther Phys Biol. 1970. 9:302–310.
Article12. Deschler DG, Kaplan MJ, Boles R. Treatment of large juvenile nasopharyngeal angiofibroma. Otolaryngol Head Neck Surg. 1992. 106:278–284.
Article13. Krekorian EA, Kato RH. Surgical management of nasopharyngeal angiofibroma with intracranial extension. Laryngoscope. 1977. 87:154–164.
Article14. Nicolai P, Berlucchi M, Tomenzoli D, Cappiello J, Trimarchi M, Maroldi R, Battaglia G, Antonelli AR. Endoscopic surgery for juvenile angiofibroma: When and how. Laryngoscope. 2003. 113:775–782.
Article15. Park KS, Lee YG, Park HS, Kim JB. Radiation-induced osteosarcoma: report of a case. J Korean Assoc Maxillofac Plast Reconstr Surg. 1998. 20:379–382.16. Cummings BJ. Relative risk factors in the treatment of juvenile nasopharyngeal angiofibroma. Head Neck Surg. 1980. 3:21–26.
Article17. Harwood AR, Cummings BJ, Fitzpatrick PJ. Radiotherapy: tumors of the head and neck. J Otolaryngol. 1984. 13:391–394.18. Dare AO, Gibbons KJ, Proulx GM, Fenstermaker RA. Resection followed by radiosurgery for advanced juvenile nasopharyngeal angiofibroma: report of two cases. Neurosurgery. 2003. 52:1207–1211.
Article19. Kuppersmith RB, Teh BS, Donovan DT, Mai WY, Chiu JK, Woo SY, Butler EB. The use of intensity modulated radiotherapy for the treatment of extensive and recurrent juvenile angiofibroma. Int J Pediatr Otorhinolaryngol. 2000. 52:261–268.
Article20. Benk V, Clark BG, Souhami L, Algan O, Bahary J, Podgorsak EB, Freeman CR. Stereotactic radiation in primary brain tumors in children and adolescents. Pediatr Neurosurg. 1999. 31:59–64.
Article21. McCombe A, Lund VJ, Howard DJ. Recurrence in juvenile angiofibroma. Rhinology. 1990. 28:97–102.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Postoperative Residual Juvenile Nasopharyngeal Angiofibroma Treated with Gamma Knife Surgery
- A Case of Juvenile Nasopharyngeal Angiofibroma-Transnasal Endoscopic Surgery-
- A Case of Juvenile Nasopharyngeal Angiofibroma Treated by Unilateral Facial Degloving Approach
- Transnasal Endoscopic Resection of Juvenile Nasopharyngeal Angiofibroma: A Case Report
- Clinical Applications of 68Ga-PSMA PET/CT on Residual Disease Assessment of Juvenile Nasopharyngeal Angiofibroma (JNA)
