J Korean Med Sci.
2006 Aug;21(4):765-767. 10.3346/jkms.2006.21.4.765.
A Case of Hyperglycemic Hyperosmolar State Associated with Graves' Hyperthyroidism: A Case Report
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Gyeongsang National University, Korea. jrhahm@gshp.gsnu.ac.kr
- 2Department of Laboratory Medicine, College of Medicine, Gyeongsang National University, Korea.
- 3Department of Biochemistry, College of Medicine, Gyeongsang National University, Korea.
- 4Gyeongsang Institute of Health Science, Jinju, Korea.
- 5Department of Laboratory Medicine, Seoul National University Hospital, Seoul, Korea.
- KMID: 2157837
- DOI: http://doi.org/10.3346/jkms.2006.21.4.765
Abstract
- Hyperglycemic hyperosmolar state (HHS) is an acute complication mostly occurring in elderly type 2 diabetes mellitus (DM). Thyrotoxicosis causes dramatic increase of glycogen degradation and/or gluconeogenesis and enhances breakdown of triglyc-erides. Thus, in general, it augments glucose intolerance in diabetic patients. A 23-yr-old female patient with Graves' disease and type 2 DM, complying with methimazole and insulin injection, had symptoms of nausea, polyuria and generalized weakness. Her serum glucose and osmolarity were 32.7 mM/L, and 321 mosm/kg, respectively. Thyroid function tests revealed that she had more aggravated hyperthyroid status; 0.01 mU/L TSH and 2.78 pM/L free T3 (reference range, 0.17-4.05, 0.31-0.62, respectively) than when she was discharged two weeks before (0.12 mU/L TSH and 1.41 pM/L free T3). Being diagnosed as HHS and refractory Graves' hyperthyroidism, she was treated successfully with intravenous fluids, insulin and high doses of methimazole (90 mg daily). Here, we described the case of a woman with Graves' disease and type 2 DM developing to HHS.
Keyword
MeSH Terms
Figure
-
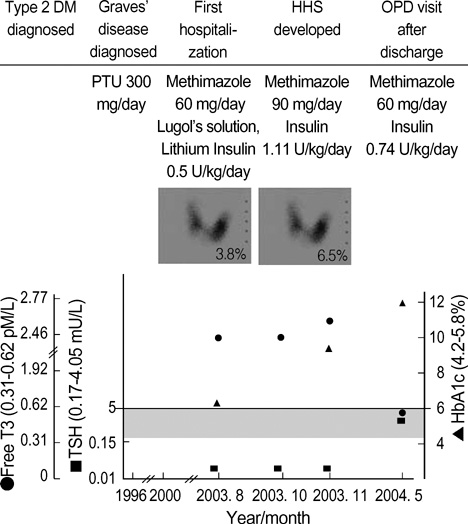
Fig. 1 The clinical course and laboratory data of this patient.
Reference
-
1. Alvin CP. Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL, Isselbacher KJ, editors. Diabetes mellitus. Harrison's Principles of Internal Medicine. 2004. 16th ed. McGraw-Hill;2152–2180.2. Bhattacharyya A, Wiles PG. Diabetic ketoacidosis precipitated by thyrotoxicosis. Postgrad Med J. 1999. 75:291–292.
Article3. Sola E, Morillas C, Garzon S, Gomez-Balaguer M, Hernandez-Mijares A. Association between diabetic ketoacidosis and thyrotoxicosis. Acta Diabetol. 2002. 39:235–237.4. Kunishige M, Sekimoto E, Komatsu M, Bando Y, Uehara M, Izumi K. Thyrotoxicosis masked by diabetic ketoacidosis: a fatal complication. Diabetes Care. 2001. 24:171.
Article5. Gomez-Balaguer M, Saurina J, Gilsanz A, Alonso C. Non-ketoacidic hyperosmolar diabetic decompensation caused by hyperthyroidism. An infrequent fact. Med Clin (Barc). 1990. 94:116–117.6. Randin J, Tappy L, Scazziga B, Jequier E, Felber J. Insulin sensitivity and exogenous insulin clearance in Graves' disease. Measurement by the glucose clamp technique and indirect calorimetry. Diabetes. 1986. 35:178–181.7. Morrison W, Gibson J, Jung R, Rennie M. Skeletal muscle and whole body protein turnover in thyroid disease. Eur J Clin Invest. 1998. 18:62–68.
Article8. Beylot M, Martin C, Laville M, Riou JP, Cohen R, Mornex R. Lipolytic and ketogenic fluxes in human hyperthyroidism. J Clin Endocrinol Metab. 1991. 73:42–49.
Article9. Loeb JN. Braverman LE, Utiger RD, editors. Metabolic changes in thyrotoxicosis. Werner and Ingbar's The thyroid. 1996. Philadelphia: Lippincott-Raven;687–693.10. Foss MC, Paccola GM, Saad MJ, Pimenta WP, Piccinato CE, Iazigi N. Peripheral glucose metabolism in human hyperthyroidism. J Clin Endocrinol Metab. 1990. 70:1167–1172.
Article11. Utiger RD. Felig P, Baxter JD, Frohman LA, editors. The thyroid: physiology, thyrotoxicosis, hypothyroidism, and the painful thyroid. Endocrinology and metabolism. 1995. New York: McGraw-Hill;435–519.12. Hagenfeldt L, Wennlund A, Felig P, Wahren J. Turnover and splanchnic metabolism of free fatty acids in hyperthyroid patients. J Clin Invest. 1981. 67:1672–1677.
Article13. Nijs HG, Radder JK, Foolich M, Krans HM. Increased insulin action and clearance in hyperthyroid newly diagnosed IDDM patient. Restoration to normal with antithyroid treatment. Diabetes Care. 1989. 12:319–324.
Article14. Wilson R, McKillop JH, Crocket GT, Pearson C, Jenkins C, Burns F, Burnett AK, Thopson JA. The effects of lithium therapy on parameters thought to be involved in the development of autoimmune thyroid disease. Clin Endocrinol (Oxf). 1991. 34:357–361.15. Fradkin JE, Wolff J. Iodide-induced thyrotoxicosis. Medicine. 1983. 62:1–20.
Article16. Landsberg L. Catecholamines and hyperthyroidism. Clin Endocrinol Metab. 1977. 6:697–718.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ocular Flutter in Hyperosmolar Hyperglycemic State during Treatment of Malignant Cerebral Edema
- Hyperglycemic Hyperosmolar State in Children with Type 2 Diabetes Mellitus: A Report of Two Cases
- Newly Diagnosed Diabetes Mellitus With Pancreatic Cancer Manifested as Hyperglycemic Hyperosmolar State
- Diabetic Ketoacidosis with Hyperglycemic Hyperosmolar State at the Onset of Type 2 Diabetes Mellitus in an Adolescent Male
- Hyperglycemic hyperosmolar state associated with invasive rhino-orbital aspergillosis in a patient with end-stage renal disease
