Common Postmortem Computed Tomography Findings Following Atraumatic Death: Differentiation between Normal Postmortem Changes and Pathologic Lesions
- Affiliations
-
- 1Department of Radiology, Graduate School of Medicine, The University of Tokyo, Tokyo 113-8655, Japan. masanoriishida@hotmail.com
- 2Department of Radiology, Mutual Aid Association for Tokyo Metropolitan Teachers and Officials, Sanraku Hospital, Tokyo 101-8326, Japan.
- 3Department of Pathology, Graduate School of Medicine, The University of Tokyo, Tokyo 113-8655, Japan.
- KMID: 2155553
- DOI: http://doi.org/10.3348/kjr.2015.16.4.798
Abstract
- Computed tomography (CT) is widely used in postmortem investigations as an adjunct to the traditional autopsy in forensic medicine. To date, several studies have described postmortem CT findings as being caused by normal postmortem changes. However, on interpretation, postmortem CT findings that are seemingly due to normal postmortem changes initially, may not have been mere postmortem artifacts. In this pictorial essay, we describe the common postmortem CT findings in cases of atraumatic in-hospital death and describe the diagnostic pitfalls of normal postmortem changes that can mimic real pathologic lesions.
MeSH Terms
Figure
-

Fig. 1 Hypostasis and hemorrhagic lesion in brain in 35-year-old deceased woman (case 1). A. CT scan obtained 8 hours and 35 minutes after death shows obscure hypostasis in dorsal superior sagittal sinus (arrowhead) in case 1. Linear and curving high density lesions are present along falx cerebri and cerebral sulcus (arrows). B. Subsequent autopsy reveals diffuse subarachnoid hemorrhage. CT = computed tomography

Fig. 2 Three lesion patterns on postmortem CT images of brain. A. Pattern 1. CT scan of 53-year-old deceased woman obtained 1 hour and 35 minutes after death shows unremarkable postmortem changes (case 2). B. Pattern 2. CT scan of 39-year-old deceased woman obtained 9 hours and 9 minutes after death shows diffuse brain swelling (case 3). C. Pattern 3. CT scan of 78-year-old deceased man obtained 14 hours and 41 minutes after death shows both diffuse brain swelling and loss of distinction between gray and white matter (case 4). CT = computed tomography

Fig. 3 Hypostasis and thrombosis in great vessels in 45-year-old deceased man (case 5). CT scan obtained 2 hours and 8 minutes after death shows hypostasis in thoracic aorta (A, arrow). Hyperdense cast is present within left pulmonary artery (A, arrowheads), which is later diagnosed as pulmonary thrombus on autopsy (B, arrow). CT = computed tomography
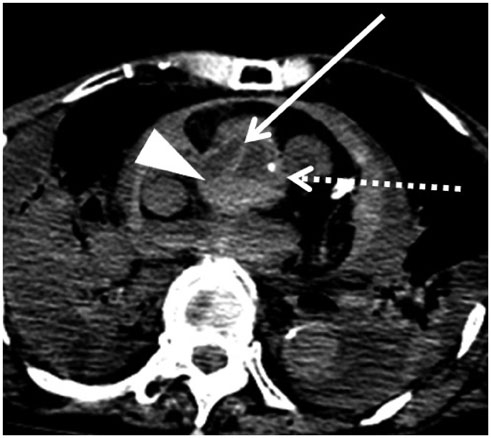
Fig. 4 Dissection and hypostasis in ascending aorta in 76-year-old deceased woman (case 6). CT scan obtained 14 hours and 30 minutes after death shows both flap (arrow) separating two lumens and hypostasis (arrowhead) in ascending aorta. Increased density and thickening of aortic wall, which are normal postmortem changes, are also observed (dotted arrow). CT = computed tomography
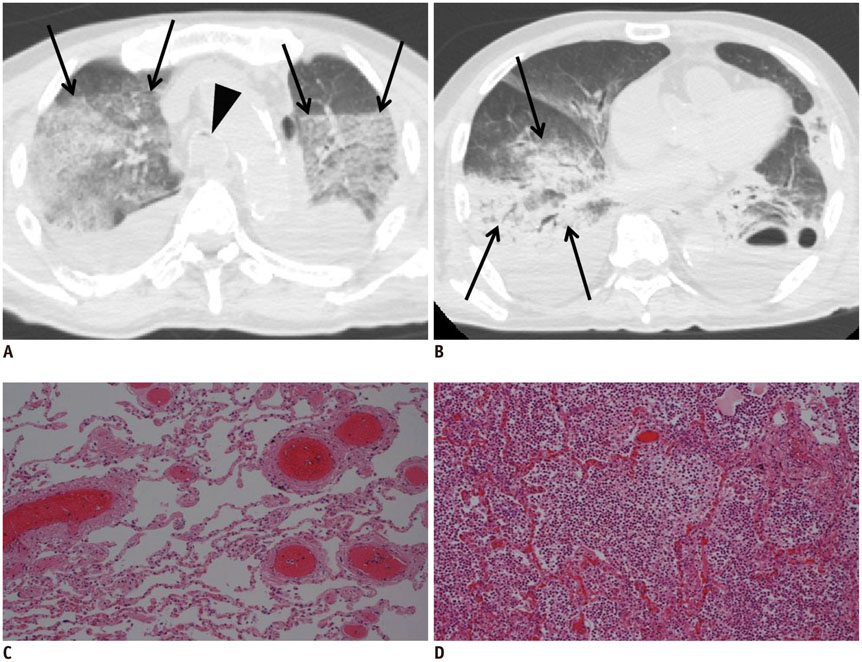
Fig. 5 Hypostasis and pathologic lesion in lung in 73-year-old deceased man (case 7). A. CT scan obtained 16 hours and 48 minutes after death shows increased density lesion with horizontal border in dependent region of left upper lobe, which is attributed to hypostasis (arrows). Endotracheal fluid, thought to be normal postmortem change, is also observed (arrowhead). B. Asymmetrical and segmental consolidation is simultaneously observed in right lower lobe (arrows). C, D. Pathological examination with hematoxylin and eosin on subsequent autopsy indicates pulmonary congestion (C; low-power view) and inflammatory cellular infiltration (pneumonia) (D; low-power view). Images C and D correspond to A and B, respectively. CT = computed tomography

Fig. 6 Hyperdense lung lesion not attributed to normal postmortem change in 18-year-old deceased man (case 8). CT scan obtained 3 hours and 32 minutes after death shows multiple areas of consolidation and randomly distributed nodules. Subsequent autopsy revealed pneumonia. CT = computed tomography
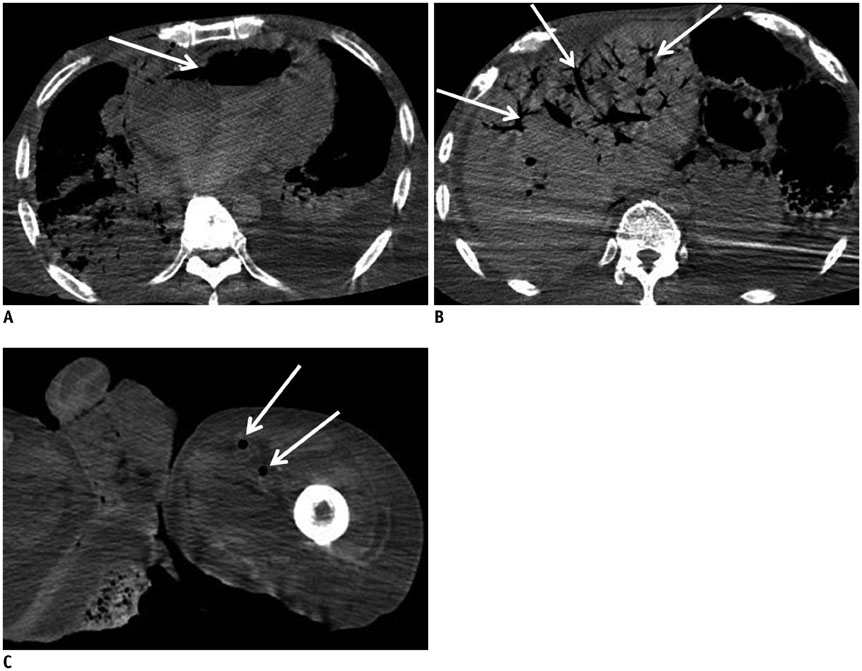
Fig. 7 Broad intraorganic/vascular gas unassociated with cardiopulmonary resuscitation (CPR) in 65-year-old deceased man (case 9). CT scan obtained 12 hours and 20 minutes after death shows intraorganic/vascular gas throughout body (A-C, arrows). Gas is observed within lumens of right atrium and ventricle (A), and left femoral artery and vein (C). Intrahepatic gas is also observed (B), which is considered to be in hepatic vascular system. CPR was not performed because patient had do-not-resuscitate order. CT = computed tomography
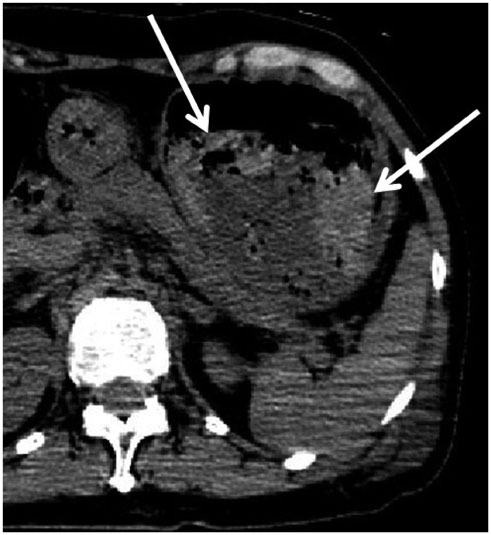
Fig. 8 Hemorrhagic hyperdense fluid in stomach in 65-year-old deceased woman with liver cirrhosis and esophagogastric varices (case 10). CT scan obtained 13 hours and 33 minutes after death shows content with two different densities in gastric lumen. Higher density material in gastric lumen (arrows) is clumped, covers lower density material, and is suspected to be caused by rupture of esophagogastric varices. This was proven on subsequent autopsy. CT = computed tomography
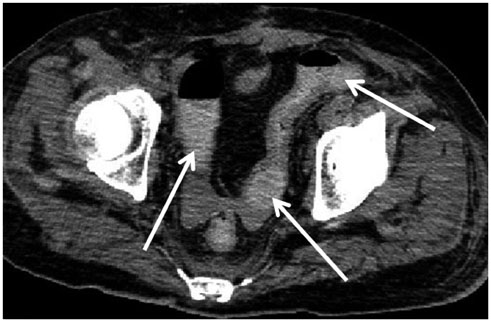
Fig. 9 Hemorrhagic hyperdense fluid in colon in 50-year-old deceased woman (case 11). CT scan obtained 2 hours and 17 minutes after death shows hyperdense contents, which fill colon (arrows) and were diagnosed as hemorrhagic on autopsy. Upon reviewing patient's medical history, we found that he was receiving anticoagulant medication and thus was at risk of hemorrhage. CT = computed tomography

Fig. 10 Non-hemorrhagic hyperdense fluid in colon in 72-year-old deceased woman (case 12). CT scan obtained 1 hours and 48 minutes after death shows hyperdense content in colon (arrow) similar to case 11. However, this material was not hemorrhagic on subsequent autopsy. It was unclear based on patient's medical history whether she was administered oral contrast medium or other oral medication, such as laxative. Residual contrast material is also observed in kidneys of cases 12 and 16 because contrast-enhanced CT was performed immediately before death. CT = computed tomography
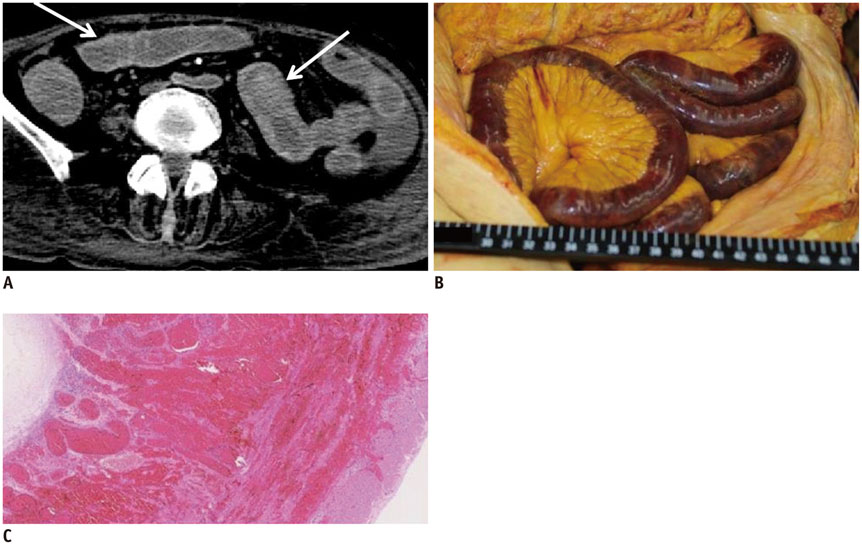
Fig. 11 Hyperdense wall of GI tract in 74-year-old deceased woman (case 13). A. CT scan obtained 2 hours and 34 minutes after death shows hyperdense walls throughout GI tract (arrows). B, C. Autopsy revealed that hyperdense GI wall was intramural hemorrhage (B, macroscopic image; C, microscopic low-power view image with hematoxylin and eosin stain). CT = computed tomography, GI = gastrointestinal

Fig. 12 Intraluminal gas in GI tract unassociated with CPR in 64-year-old deceased man (case 14). CT scan obtained 3 hours and 57 minutes after death shows widespread distension of GI tract. Although this finding can be caused by CPR, in this patient, CPR was not performed due to DNR order. This finding is considered nonspecific. CPR = cardiopulmonary resuscitation, CT = computed tomography, DNR = do-not-resuscitate, GI = gastrointestinal
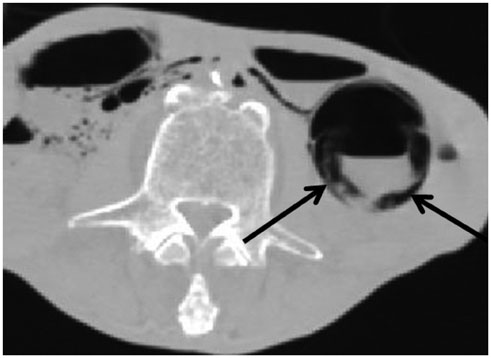
Fig. 13 Intramural gas in GI tract caused by antemortem condition in 75-year-old deceased man who underwent CPR (case 15). CT scan obtained 4 hours and 21 minutes after death shows intramural gas throughout GI tract (arrows). Although there may have some contribution from CPR, autopsy proved that he had pneumatosis cystoides intestinalis. CT = computed tomography, GI = gastrointestinal

Fig. 14 Intramural gas in GI tract unassociated with CPR in 72-year-old deceased woman who did not undergo CPR (case 16). CT scan obtained 1 hour and 48 minutes after death shows intramural gas throughout GI tract (arrows) similar to case 15. CPR was not performed before death due to patient's DNR order. However, autopsy did not reveal any pathology associated with this postmortem CT finding. Therefore, intramural gas was attributed to mucosal injury, which is normal postmortem change. CPR = cardiopulmonary resuscitation, CT = computed tomography, DNR = do-not-resuscitate, GI = gastrointestinal
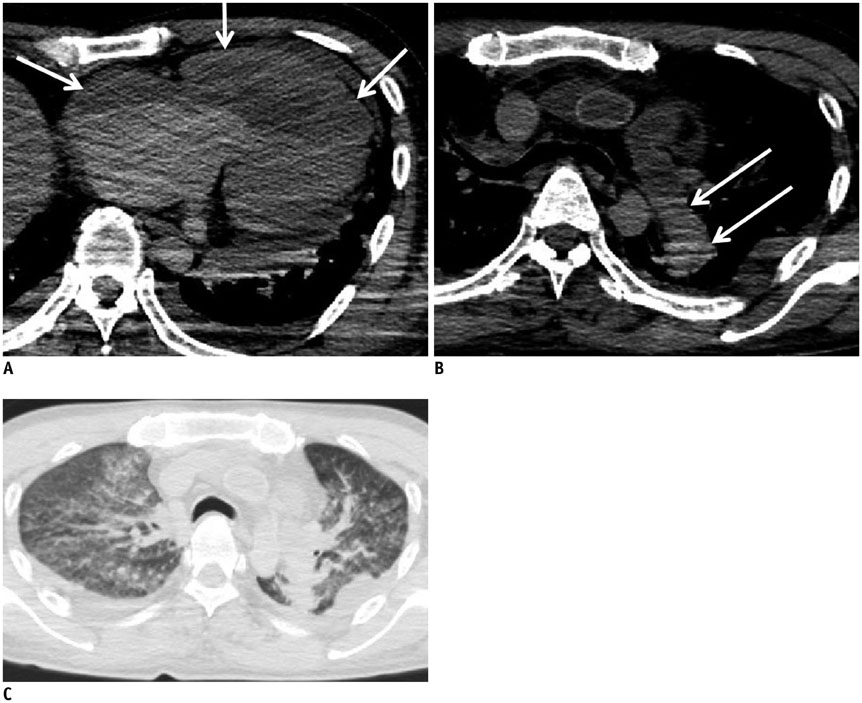
Fig. 15 Dilatation of right heart in 50-year-old deceased man (case 17). CT scan obtained 17 hours and 18 minutes after death shows dilatation of right heart (A, arrows). Although this is known to be normal postmortem change caused by blood congestion, it became clear with in autopsy that finding in this case was caused by pulmonary veno-occlusive disease. Other lesions related to this disease are also present: pulmonary artery dilation (B, arrows) and pulmonary edema (C). CT = computed tomography
Reference
-
1. Patriquin L, Kassarjian A, Barish M, Casserley L, O'Brien M, Andry C, et al. Postmortem whole-body magnetic resonance imaging as an adjunct to autopsy: preliminary clinical experience. J Magn Reson Imaging. 2001; 13:277–287.2. Thali MJ, Yen K, Schweitzer W, Vock P, Boesch C, Ozdoba C, et al. Virtopsy, a new imaging horizon in forensic pathology: virtual autopsy by postmortem multislice computed tomography (MSCT) and magnetic resonance imaging (MRI)--a feasibility study. J Forensic Sci. 2003; 48:386–403.3. Ezawa H, Yoneyama R, Kandatsu S, Yoshikawa K, Tsujii H, Harigaya K. Introduction of autopsy imaging redefines the concept of autopsy: 37 cases of clinical experience. Pathol Int. 2003; 53:865–873.4. Roberts IS, Benamore RE, Benbow EW, Lee SH, Harris JN, Jackson A, et al. Post-mortem imaging as an alternative to autopsy in the diagnosis of adult deaths: a validation study. Lancet. 2012; 379:136–142.5. Shiotani S, Kohno M, Ohashi N, Yamazaki K, Nakayama H, Watanabe K, et al. Non-traumatic postmortem computed tomographic (PMCT) findings of the lung. Forensic Sci Int. 2004; 139:39–48.6. Aghayev E, Sonnenschein M, Jackowski C, Thali M, Buck U, Yen K, et al. Postmortem radiology of fatal hemorrhage: measurements of cross-sectional areas of major blood vessels and volumes of aorta and spleen on MDCT and volumes of heart chambers on MRI. AJR Am J Roentgenol. 2006; 187:209–215.7. Jackowski C, Schweitzer W, Thali M, Yen K, Aghayev E, Sonnenschein M, et al. Virtopsy: postmortem imaging of the human heart in situ using MSCT and MRI. Forensic Sci Int. 2005; 149:11–23.8. Kobayashi T, Shiotani S, Kaga K, Saito H, Saotome K, Miyamoto K, et al. Characteristic signal intensity changes on postmortem magnetic resonance imaging of the brain. Jpn J Radiol. 2010; 28:8–14.9. Ishida M, Gonoi W, Hagiwara K, Takazawa Y, Akahane M, Fukayama M, et al. Postmortem changes of the thyroid on computed tomography. Leg Med (Tokyo). 2011; 13:318–332.10. Ishida M, Gonoi W, Hagiwara K, Okuma H, Shirota G, Shintani Y, et al. Early postmortem volume reduction of adrenal gland: initial longitudinal computed tomographic study. Radiol Med. 2015; 120:662–669.11. Shiotani S, Takahashi N, Anzai Y, Hasegawa I, Yamamoto S, Oguma E, et al. Guidelines for interpretation of postmortem CT. In : Imai Y, Takano H, Yamamoto S, editors. Autopsy imaging guideline. 2nd ed. Tokyo: Vector Core;2012. p. 54–68.12. Okuma H, Gonoi W, Ishida M, Shintani Y, Takazawa Y, Fukayama M, et al. Heart wall is thicker on postmortem computed tomography than on antemortem [corrected] computed tomography: the first longitudinal study. PLoS One. 2013; 8:e76026.13. Okuma H, Gonoi W, Ishida M, Shirota G, Shintani Y, Abe H, et al. Comparison of attenuation of striated muscle between postmortem and antemortem computed tomography: results of a longitudinal study. PLoS One. 2014; 9:e111457.14. Jackowski C, Thali MJ, Buck U, Aghayev E, Sonnenschein M, Yen K, et al. Noninvasive estimation of organ weights by postmortem magnetic resonance imaging and multislice computed tomography. Invest Radiol. 2006; 41:572–578.15. Ishida M, Gonoi W, Hagiwara K, Takazawa Y, Akahane M, Fukayama M, et al. Intravascular gas distribution in the upper abdomen of non-traumatic in-hospital death cases on postmortem computed tomography. Leg Med (Tokyo). 2011; 13:174–179.16. Ishida M, Gonoi W, Hagiwara K, Takazawa Y, Akahane M, Fukayama M, et al. Hypostasis in the heart and great vessels of non-traumatic in-hospital death cases on postmortem computed tomography: relationship to antemortem blood tests. Leg Med (Tokyo). 2011; 13:280–285.17. Ishida M, Gonoi W, Hagiwara K, Okuma H, Shintani Y, Abe H, et al. Fluid in the airway of nontraumatic death on postmortem computed tomography: relationship with pleural effusion and postmortem elapsed time. Am J Forensic Med Pathol. 2014; 35:113–117.18. Okuma H, Gonoi W, Ishida M, Shintani Y, Takazawa Y, Fukayama M, et al. Greater thickness of the aortic wall on postmortem computed tomography compared with antemortem computed tomography: the first longitudinal study. Int J Legal Med. 2014; 128:987–993.19. Cha JG, Kim DH, Kim DH, Paik SH, Park JS, Park SJ, et al. Utility of postmortem autopsy via whole-body imaging: initial observations comparing MDCT and 3.0 T MRI findings with autopsy findings. Korean J Radiol. 2010; 11:395–406.20. Levy AD, Harcke HT, Mallak CT. Postmortem imaging: MDCT features of postmortem change and decomposition. Am J Forensic Med Pathol. 2010; 31:12–17.21. Shepherd R. Simpson's forensic medicine. 12th ed. London: Arnold;2003. p. 37–41.22. Di Maio VJ, Di Maio DJ. Forensic pathology. 2nd ed. Boca Raton: CRC Press;2001. p. 21–26.23. Payne-James J, Busuttil A, Smock W. Forensic medicine: clinical and pathological aspects. 1st ed. San Francisco: Greenwich Medical Media;2002. p. 731–746.24. Shiotani S, Kohno M, Ohashi N, Yamazaki K, Itai Y. Postmortem intravascular high-density fluid level (hypostasis): CT findings. J Comput Assist Tomogr. 2002; 26:892–893.25. Jackowski C, Thali M, Aghayev E, Yen K, Sonnenschein M, Zwygart K, et al. Postmortem imaging of blood and its characteristics using MSCT and MRI. Int J Legal Med. 2006; 120:233–240.26. Takahashi N, Satou C, Higuchi T, Shiotani M, Maeda H, Hirose Y. Quantitative analysis of intracranial hypostasis: comparison of early postmortem and antemortem CT findings. AJR Am J Roentgenol. 2010; 195:W388–W393.27. Takahashi N, Satou C, Higuchi T, Shiotani M, Maeda H, Hirose Y. Quantitative analysis of brain edema and swelling on early postmortem computed tomography: comparison with antemortem computed tomography. Jpn J Radiol. 2010; 28:349–354.28. Smith AB, Lattin GE Jr, Berran P, Harcke HT. Common and expected postmortem CT observations involving the brain: mimics of antemortem pathology. AJNR Am J Neuroradiol. 2012; 33:1387–1391.29. Dedouit F, Sévely A, Costagliola R, Otal P, Loubes-Lacroix F, Manelfe C, et al. Reversal sign on ante- and postmortem brain imaging in a newborn: report of one case. Forensic Sci Int. 2008; 182:e11–e14.30. Kjos BO, Brant-Zawadzki M, Young RG. Early CT findings of global central nervous system hypoperfusion. AJR Am J Roentgenol. 1983; 141:1227–1232.31. Bird CR, Drayer BP, Gilles FH. Pathophysiology of "reverse" edema in global cerebral ischemia. AJNR Am J Neuroradiol. 1989; 10:95–98.32. Han BK, Towbin RB, De Courten-Myers G, McLaurin RL, Ball WS Jr. Reversal sign on CT: effect of anoxic/ischemic cerebral injury in children. AJNR Am J Neuroradiol. 1989; 10:1191–1198.33. Sieswerda-Hoogendoorn T, Beenen LF, van Rijn RR. Normal cranial postmortem CT findings in children. Forensic Sci Int. 2015; 246:43–49.34. Jackowski C, Grabherr S, Schwendener N. Pulmonary thrombembolism as cause of death on unenhanced postmortem 3T MRI. Eur Radiol. 2013; 23:1266–1270.35. Tatco VR, Piedad HH. The validity of hyperdense lumen sign in non-contrast chest CT scans in the detection of pulmonary thromboembolism. Int J Cardiovasc Imaging. 2011; 27:433–440.36. Cobelli R, Zompatori M, De Luca G, Chiari G, Bresciani P, Marcato C. Clinical usefulness of computed tomography study without contrast injection in the evaluation of acute pulmonary embolism. J Comput Assist Tomogr. 2005; 29:6–12.37. Shiotani S, Kohno M, Ohashi N, Yamazaki K, Nakayama H, Ito Y, et al. Hyperattenuating aortic wall on postmortem computed tomography (PMCT). Radiat Med. 2002; 20:201–206.38. Takahashi N, Higuchi T, Hirose Y, Yamanouchi H, Takatsuka H, Funayama K. Changes in aortic shape and diameters after death: comparison of early postmortem computed tomography with antemortem computed tomography. Forensic Sci Int. 2013; 225:27–31.39. Hyodoh H, Sato T, Onodera M, Washio H, Hasegawa T, Hatakenaka M. Vascular measurement changes observed using postmortem computed tomography. Jpn J Radiol. 2012; 30:840–845.40. Shiotani S, Kobayashi T, Hayakawa H, Kikuchi K, Kohno M. Postmortem pulmonary edema: a comparison between immediate and delayed postmortem computed tomography. Leg Med (Tokyo). 2011; 13:151–155.41. Takahashi N, Higuchi T, Shiotani M, Maeda H, Hirose Y. Intrahepatic gas at postmortem multislice computed tomography in cases of nontraumatic death. Jpn J Radiol. 2009; 27:264–268.42. Jackowski C, Sonnenschein M, Thali MJ, Aghayev E, Yen K, Dirnhofer R, et al. Intrahepatic gas at postmortem computed tomography: forensic experience as a potential guide for in vivo trauma imaging. J Trauma. 2007; 62:979–988.43. Shiotani S, Kohno M, Ohashi N, Yamazaki K, Nakayama H, Watanabe K. Postmortem computed tomographic (PMCT) demonstration of the relation between gastrointestinal (GI) distension and hepatic portal venous gas (HPVG). Radiat Med. 2004; 22:25–29.44. Asamura H, Ito M, Takayanagi K, Kobayashi K, Ota M, Fukushima H. Hepatic portal venous gas on postmortem CT scan. Leg Med (Tokyo). 2005; 7:326–333.45. Shiotani S, Kohno M, Ohashi N, Atake S, Yamazaki K, Nakayama H. Cardiovascular gas on non-traumatic postmortem computed tomography (PMCT): the influence of cardiopulmonary resuscitation. Radiat Med. 2005; 23:225–229.46. Yamaki T, Ando S, Ohta K, Kubota T, Kawasaki K, Hirama M. CT demonstration of massive cerebral air embolism from pulmonary barotrauma due to cardiopulmonary resuscitation. J Comput Assist Tomogr. 1989; 13:313–315.47. Hwang SL, Lieu AS, Lin CL, Liu GC, Howng SL, Kuo TH. Massive cerebral air embolism after cardiopulmonary resuscitation. J Clin Neurosci. 2005; 12:468–469.48. Sakata M, Miki A, Kazama H, Morita M, Yasoshima S. Studies on the composition of gases in the post-mortem body: animal experiments and two autopsy cases. Forensic Sci Int. 1980; 15:19–29.49. Singh MK, O'Donnell C, Woodford NW. Progressive gas formation in a deceased person during mortuary storage demonstrated on computed tomography. Forensic Sci Med Pathol. 2009; 5:236–242.50. Gill JR, Landi K. Putrefactive rigor: apparent rigor mortis due to gas distension. Am J Forensic Med Pathol. 2011; 32:242–244.51. Spitz WU, Spitz DJ, Fisher RS. Spitz and Fisher's Medicolegal Investigation of Death: Guidelines for the Application of Pathology to Crime Investigation. 4th ed. Springfield: Charles C Thomas;2006. p. 108.52. Shiotani S, Ueno Y, Atake S, Kohno M, Suzuki M, Kikuchi K, et al. Nontraumatic postmortem computed tomographic demonstration of cerebral gas embolism following cardiopulmonary resuscitation. Jpn J Radiol. 2010; 28:1–7.53. Chou CK, Mak CW, Tzeng WS, Chang JM. CT of small bowel ischemia. Abdom Imaging. 2004; 29:18–22.54. Benson MD. Adult survival with intrahepatic portal venous gas secondary to acute gastric dilatation, with a review of portal venous gas. Clin Radiol. 1985; 36:441–443.55. Edlich RF, Borner JW, Kuphal J. Gastric blood flow: its destruction during gastric distention. Am J Surg. 1976; 120:635–640.56. Christe A, Flach P, Ross S, Spendlove D, Bolliger S, Vock P, et al. Clinical radiology and postmortem imaging (Virtopsy) are not the same: specific and unspecific postmortem signs. Leg Med (Tokyo). 2010; 12:215–222.57. Shiotani S, Kohno M, Ohashi N, Yamazaki K, Nakayama H, Watanabe K, et al. Dilatation of the heart on postmortem computed tomography (PMCT): comparison with live CT. Radiat Med. 2003; 21:29–35.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Discrepancies in the Cause and Manner of Death Reported in Postmortem Inspection and Autopsy
- Differences in the Determination of Cause and Manner of 127 Natural Death Cases by Postmortem Inspection and Autopsy
- Postmortem Biochemistry (I) : Cardiac Markers
- Recommendation of the Guideline for Postmortem Inspection at Scene on Forensic Aspects
- Proposal of Comprehensive Act for Postmortem Examination to Improve Death Certification System
