Axial Torsion of Meckel's Diverticulum Causing Small Bowel Obstruction in Adult: A Case Report
- Affiliations
-
- 1Department of Radiology, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea. ymiku@catholic.ac.kr
- KMID: 2152604
- DOI: http://doi.org/10.3348/jksr.2016.74.2.123
Abstract
- Meckel's diverticulum (MD) is the most common congenital abnormality of the gastrointestinal tract that is prevalent in 2-3% of the population. The lifetime risk of complications is estimated at 4%. Small bowel obstruction is the second most common complication of MD. Among the causes of bowel obstruction, axial torsion of MD is the rarest complication. Urgent surgical treatment is needed in cases of small bowel obstruction associated with torsion of MD. Pre-operative diagnosis of MD as a cause of small bowel obstruction is difficult, because the diagnosis can be made only if the diverticulum is delineated at the site of obstruction. We reported a case of axial torsion of MD with necrosis that caused proximal small bowel perforation in a 21-year-old male.
MeSH Terms
Figure
-
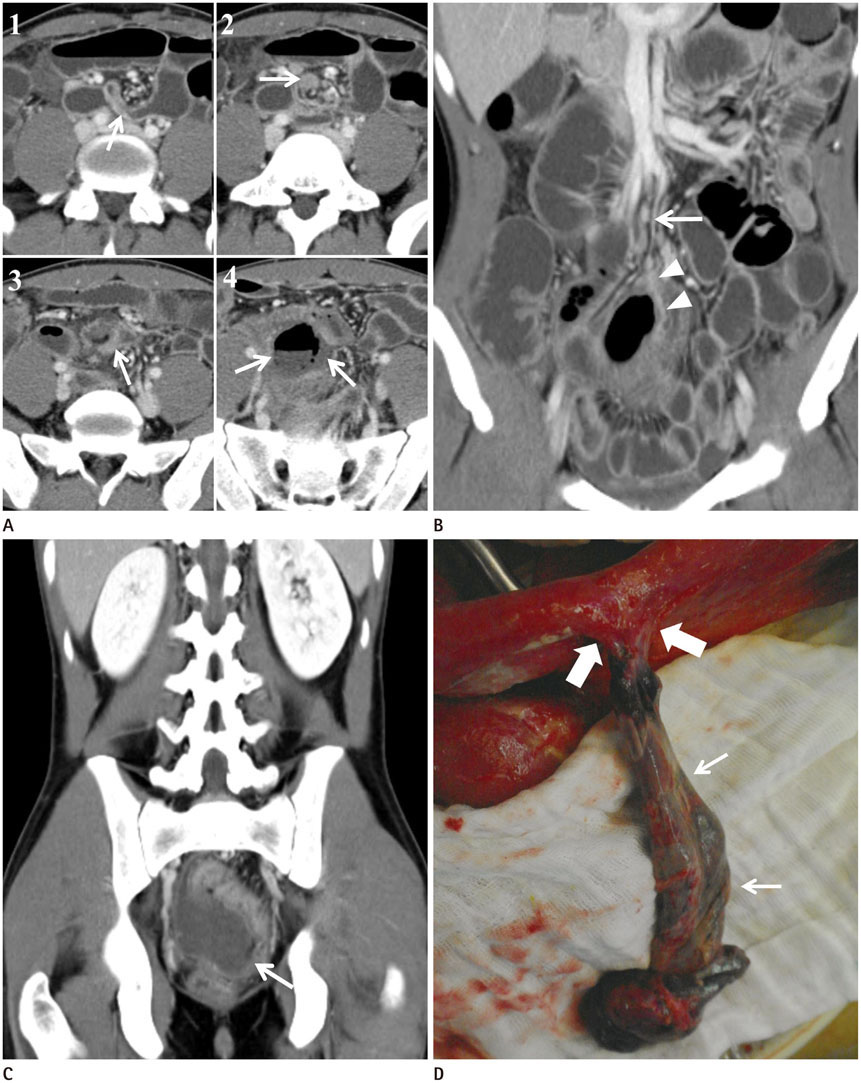
Fig. 1 A 21-year-old male patient presented a Meckel's diverticulum (MD) with axial torsion resulting in small bowel obstruction and perforation. A. Consecutive axial images (order is marked by number 1 through 4) from contrast-enhanced computed tomography demonstrate a tubular structure (arrow in 1) connected with distal ileum and axial torsion of its neck (arrows in 2 and 3). Air-fluid level is observed in the lumen of tubular structure with pneumatosis of its wall (arrows in 4). Note the dilated adjacent small bowel loops. B. On coronal reformatted image, the artery suggesting vitellointestinal artery (arrowheads) originates from ileal branch of superior mesenteric artery (arrow) and supplies the MD in distal ileum. C. Coronal reformatted image demonstrates an approximately 4.8 × 5.5 × 17.8 cm sized tubular structure, which is connected to distal ileum extending into pelvic cavity with blind-end (arrow). D. The surgical specimen is an about 20 cm-length of infarcted MD (arrows), which is connected to distal ileum (thick arrows) with gangrenous change. There is no fibrous band attached to the distal end of MD.
Reference
-
1. Levy AD, Hobbs CM. From the archives of the AFIP. Meckel diverticulum: radiologic features with pathologic Correlation. Radiographics. 2004; 24:565–558.2. Limas C, Seretis K, Soultanidis C, Anagnostoulis S. Axial torsion and gangrene of a giant Meckel's diverticulum. J Gastrointestin Liver Dis. 2006; 15:67–68.3. Murruste M, Rajaste G, Kase K. Torsion of Meckel's diverticulum as a cause of small bowel obstruction: a case report. World J Gastrointest Surg. 2014; 6:204–207.4. Akbulut S, Yagmur Y. Giant Meckel's diverticulum: an exceptional cause of intestinal obstruction. World J Gastrointest Surg. 2014; 6:47–50.5. Seth A, Seth J. Axial torsion as a rare and unusual complication of a Meckel's diverticulum: a case report and review of the literature. J Med Case Rep. 2011; 5:118.6. Jalil O, Radwan R, Rasheed A, Nutt MR. Congenital band of the vitelline artery remnant as a cause of chronic lower abdominal pain in an adult: case report. Int J Surg Case Rep. 2012; 3:207–208.7. Sasikumar K, Noonavath RN, Sreenath GS, Maroju NK. Axial torsion of gangrenous Meckel's diverticulum causing small bowel obstruction. J Surg Tech Case Rep. 2013; 5:103–105.8. Cartanese C, Petitti T, Marinelli E, Pignatelli A, Martignetti D, Zuccarino M, et al. Intestinal obstruction caused by torsed gangrenous Meckel's diverticulum encircling terminal ileum. World J Gastrointest Surg. 2011; 3:106–109.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intestinal Obstruction Due to a Torsional Huge Meckel's Diverticulum
- Laparoscopic Treatment of Gangrene of Giant Meckel's Diverticulum Secondary to Axial Torsion
- Laparoscopic Management for Intestinal Obstruction Caused by Meckel's Diverticulum
- A Case of Recurrent Intestinal Obstruction Caused by Meckel's Diverticulum
- Small Bowel Infarction Caused by Mesodiverticular Band and Meckel's Diverticulum : A Case Report
