A Case of Non ST Elevation Myocardial Infarction by Coronary Artery Focal Spasm in a Patient with Autosomal Dominant Polycystic Kidney Disease
- Affiliations
-
- 1Department of Internal Medicine, Busan Medical Center, Busan, Korea. yoplait83@hanmail.net
- KMID: 2151824
- DOI: http://doi.org/10.12997/jla.2015.4.2.145
Abstract
- Autosomal dominant polycystic kidney disease (ADPKD) is the most common inherited renal disease. The main causes of death in ADPKD are cardiovascular disease as well as infections and neurological reasons. ADPKD is causing vasculopathy including aortic root dilation, cerebral artery aneurysm, coronary aneurysm, and aortic dissection. In this case report, we describe a 37-year-old female ADPKD patient with non-ST elevation MI (NSTEMI) caused by coronary artery focal spasm.
Keyword
MeSH Terms
Figure
-

Fig. 1 Computed-tomography (CT) scans during the first visit. CT shows that both kidneys have polycystics. (A) Horizontal view, (B) Coronal view.

Fig. 2 Echocardiography during the first visit. Apical four-chamber view shows apical Regional wall motion abnormality (RWMA) (A) and apical RWMA with ballooning (B).
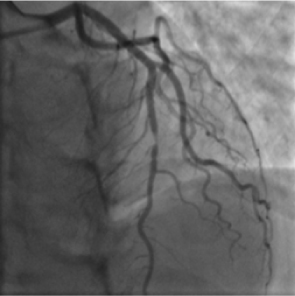
Fig. 3 Coronary angiography shows 70-80% stenosis in the mid left anterior descending coronary artery.
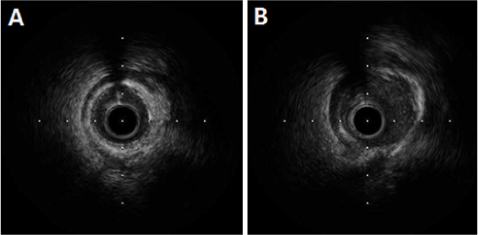
Fig. 4 Intravascular ultrasound. (A) Before injection of nitroglycerin in patient with coronary artery. External elastic membrane (EEM) cross-sectional area (CSA): 4.7 mm2, lumen CSA: 3.7 mm2, 21% stenosis (plaque area/EEM CSA), (B) After injection of nitroglycerin in patient with coronary artery. EEM CSA: 7.15mm2, lumen CSA: 4.76mm2, 33% stenosis.
Reference
-
1. Niemczyk M, Pilecki T, Gradzik M, Bujko M, Niemczyk S, Pączek L. Blood pressure and intracranial aneurysms in autosomal dominant polycystic kidney disease. Kidney Blood Press Res. 2014; 39:630–635.
Article2. Gabow PA. Autosomal dominant polycystic kidney disease. N Engl J Med. 1993; 329:332–342.
Article3. Fick GM, Johnson AM, Hammond WS, Gabow PA. Causes of death in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1995; 5:2048–2056.
Article4. Ecder T, Schrier RW. Cardiovascular abnormalities in autosomal-dominant polycystic kidney disease. Nat Rev Nephrol. 2009; 5:221–228.
Article5. Chapman AB, Johnson AM, Rainguet S, Hossack K, Gabow P, Schrier RW. Left ventricular hypertrophy in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1997; 8:1292–1297.
Article6. Chang MY, Ong AC. Autosomal dominant polycystic kidney disease: recent advances in pathogenesis and treatment. Nephron Physiol. 2008; 108:p1–p7.
Article7. Magadle R, Weiner P, Rabner M, Mizrahi-Reuveni M, Davidovich A. Polycystic kidney disease as a new risk factor for coronary events. Isr Med Assoc J. 2002; 4:21–23.8. Nakaike R, Urabe Y, Shimokawa H, Kinjoh M, Takeshita A. Recurrent myocardial infarction provoked by multiple giant coronary aneurysms. A case report. Angiology. 1996; 47:311–314.
Article9. Yamagishi M, Miyatake K, Tamai J, Nakatani S, Koyama J, Nissen SE. Intravascular ultrasound detection of atherosclerosis at the site of focal vasospasm in angiographically normal or minimally narrowed coronary segments. J Am Coll Cardiol. 1994; 23:352–357.
Article10. Kocyigit I, Taheri S, Sener EF, Unal A, Eroglu E, Öztürk F, et al. Endothelial nitric oxide synthase gene expression is associated with hypertension in autosomal dominant polycystic kidney disease. Cardiorenal Med. 2014; 4:269–279.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute Myocardial Infarction With ST-Segment Elevation in a Lead Augmented Right Vector Caused by a Left Main Coronary Artery Vasospasm
- A Case of Renal Cell Carcinoma in Autosomal Dominant Polycystic Kidney Disease Hemodialyzed
- Acute Myocardial Infarction by Right Coronary Artery Occlusion Presenting as Precordial ST Elevation on Electrocardiography
- Cardiogenic Shock From Global Myocardial Ischemia Induced by Simultaneous Multivessel Coronary Spasm
- Segmental Cystic Disease of the Kidney: A Case Report
