J Lipid Atheroscler.
2015 Dec;4(2):137-140. 10.12997/jla.2015.4.2.137.
Myocardial Ischemia by Aggravation of Myocardial Bridging
- Affiliations
-
- 1Division of Cardiology, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. krheart@hallym.or.kr
- KMID: 2151822
- DOI: http://doi.org/10.12997/jla.2015.4.2.137
Abstract
- Myocardial bridging (MB) occurs when the myocardium covers a segment of a major epicardial coronary artery, resulting in a tunneled arterial segment. Although MB is generally considered benign, it has been associated with myocardial ischemia. A 70-year-old man with MB (50% luminal narrowing during systole) at the mid-left anterior descending artery (LAD) on previous coronary angiography (CAG) visited our hospital with worsening chest pain. His blood pressure (BP) was not well controlled because of poor compliance. Follow-up CAG showed that MB at the mid-LAD progressed to severe stenosis (>90% luminal narrowing during systole) and the total length of tunneled artery extended from 22.5 to 23.9 mm. His chest pain was relieved by BP control. This is the first report of myocardial ischemia secondary to progression of MB demonstrated by CAG in Korea.
Keyword
MeSH Terms
Figure
-
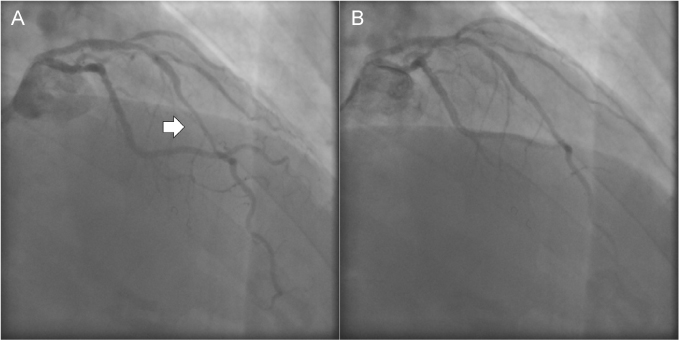
Fig. 1 Coronary angiography of the left anterior descending artery (LAD) in 2006. (A) Moderate systolic stenosis (50% luminal narrowing) was observed at end-systole, and the total length of the bridged segment was 22.5 mm (arrow). (B) The LAD at end-diastole showed no obvious stenotic lesion.
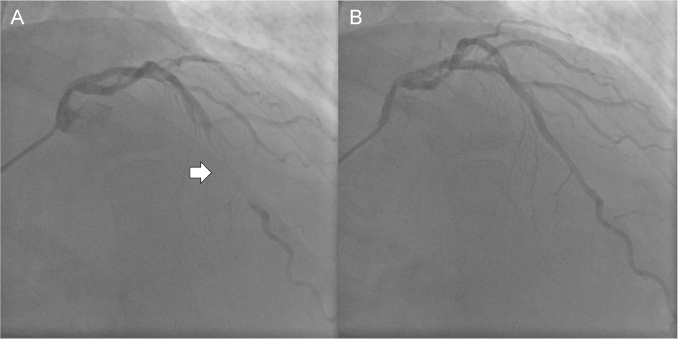
Fig. 2 Coronary angiography of the left anterior descending artery (LAD) in 2014. (A) Severe systolic stenosis (>90% luminal narrowing) was observed at end-systole, and the total length of the bridged segment was 23.9 mm (arrow). (B) The LAD at end-diastole showed no obvious stenotic lesion.
Reference
-
1. Geiringer E. The mural coronary. Am Heart J. 1951; 41:359–368.
Article2. Mazzù A, Di Tano G, Cogode R, Lo Presti G. Myocardial bridging involving more than one site of the left anterior descending coronary artery: an uncommon cause of acute ischemic syndrome. Cathet Cardiovasc Diagn. 1995; 34:329–332.
Article3. Möhlenkamp S, Hort W, Ge J, Erbel R. Update on myocardial bridging. Circulation. 2002; 106:2616–2622.
Article4. Faruqui AM, Maloy WC, Felner JM, Schlant RC, Logan WD, Symbas P. Symptomatic myocardial bridging of coronary artery. Am J Cardiol. 1978; 41:1305–1310.
Article5. Cutler D, Wallace JM. Myocardial bridging in a young patient with sudden death. Clin Cardiol. 1997; 20:581–583.
Article6. Arjomand H, AlSalman J, Azain J, Amin D. Myocardial bridging of left circumflex coronary artery associated with acute myocardial infarction. J Invasive Cardiol. 2000; 12:431–434.7. Erbel R, Rupprecht HJ, Ge J, Gerber T, Görge G, Meyer J. Coronary artery shape and flow changes induced by myocardial bridging. Echocardiography. 1993; 1:71–77.
Article8. Yano K, Yoshino H, Taniuchi M, Kachi E, Shimizu H, Watanuki A, et al. Myocardial bridging of the left anterior descending coronary artery in acute inferior wall myocardial infarction. Clin Cardiol. 2001; 24:202–208.
Article9. Masuda T, Ito K, Nagao T, Ide Y, Tsuboi H, Goto T. Myocardial bridge with progression in the short term. Circ J. 2013; 77:2152–2154.
Article10. Ishikawa Y, Kawawa Y, Kohda E, Shimada K, Ishii T. Significance of the anatomical properties of a myocardial bridge in coronary heart disease. Circ J. 2011; 75:1559–1566.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Q Wave Acute Myocardial Infarction in Patients with Myocardial Bridging Caused by Fibrous Band
- Correlation Between Functional Myocardial Perfusion Imaging and Anatomical Cardiac CT in a Case of Myocardial Bridging
- A Case of Myocardial Infarction in a Patient with Myocardial Bridge and Atrial Fibrillation
- A Case of Non-Q Myocardial Infaction in a Patient with Myocardial Bridging
- A Case of Coronary Stenting in the Management of Myocardial Ischemia Caused by Myocardial Bridging
