Hip Pelvis.
2015 Dec;27(4):278-282. 10.5371/hp.2015.27.4.278.
Compartment Syndrome of the Gluteus Medius Occurred without Bleeding or Trauma: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea. slowsting@naver.com
- KMID: 2150517
- DOI: http://doi.org/10.5371/hp.2015.27.4.278
Abstract
- Compartment syndrome is an ischemic change resulting from an increase in compartment pressure. Initially, patients present with direct tenderness and swelling, and the weak circulation secondary to compartment syndrome can eventually lead to motor and sensory impairment. If the increase in pressure results in neurological impairment, emergency intervention is required to decompress the compartment. Typically, compartment syndrome develops on forearms or lower legs. The gluteal compartment is rarely the location of compartment syndrome and only a few cases have been presented in the literature with trauma or hematoma. We have treated a patient with gluteal compartment syndrome who presented with no history of trauma or hemorrhage and present that case report here.
Keyword
Figure
-

Fig. 1 Compartment pressure measuring tool using Whitesides technique.
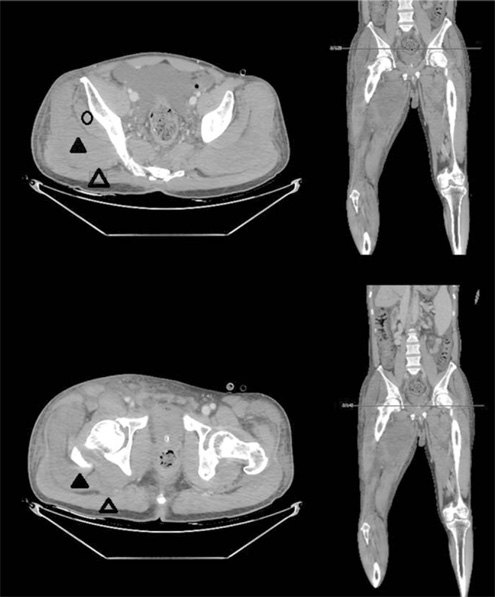
Fig. 2 Direct tenderness and severe swelling were found in the patient's right leg. Circle: gluteus minimus, black triangle: gluteus medius, empty triangle: gluteus maximus.

Fig. 3 Ischemic change and loss of contractability of gluteus medius. Black arrow: gluteus medius, white arrow: vastus lateralis.
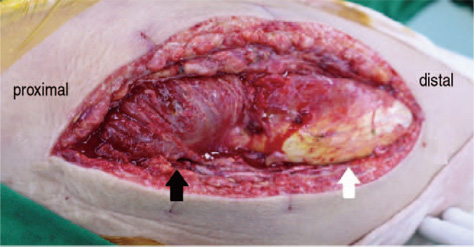
Fig. 4 Postoperative 5 days, at the second operation, the swelling of the gluteus medius subsided and ischemic changes were recovered. Black arrow: gluteus medius, white arrow: vastus lateralis.
Reference
-
1. Lee KB, Lee SH. Diagnosis and management of acute compartment syndrome. J Korean Fract Soc. 2015; 28:93–101.
Article2. Oh CW, Lee HJ. Acute compartment syndrome after trauma. J Korean Fract Soc. 2010; 23:399–403.
Article3. Petrik ME, Stambough JL, Rothman RH. Posttraumatic gluteal compartment syndrome. A case report. Clin Orthop Relat Res. 1988; (231):127–129.4. Chung KJ, Chung YK, Yoo JH, Wang JS. Sciatic nerve palsy complicating gluteal compartment syndrome due to rhabdomyolysis: a case report. J Korean Orthop Assoc. 2005; 40:103–106.
Article5. Choi DH, Choi DW, Awe SI, et al. Low molecular weight heparin associated intramuscular hematoma with compartment syndrome. Korean J Med. 2005; 69:Suppl 3. S948–S951.6. Lee MJ, Lee DK. Spontaneous multi-stage gluteus muscular hemorrhage following long-term use of clopidogrel. J Korean Neurol Assoc. 2011; 29:406.7. Ehlinger M, Schneider L, Lefebvre Y, Jacquot X, Cognet JM, Simon P. Exercise-induced acute bilateral isolated anterolateral compartment syndrome of the leg: a case report of a rare condition. Rev Chir Orthop Reparatrice Appar Mot. 2004; 90:165–170.8. Browner BD, Alberta FG, Furey PC, Goumas D, Varma V. Emergent care of musculoskeletal injuries. In : Townsend CM, Beauchamp RD, Evers DM, Mattox K, editors. Sabiston textbook of surgery. 17th ed. Philadelphia, PA: W.B. Saunders;2004. p. 554–557.9. Whitesides TE, Haney TC, Morimoto K, Harada H. Tissue pressure measurements as a determinant for the need of fasciotomy. Clin Orthop Relat Res. 1975; (113):43–51.
Article10. Owen CA, Woody PR, Mubarak SJ, Hargens AR. Gluteal compartment syndromes: a report of three cases and management utilizing the Wick catheter. Clin Orthop Relat Res. 1978; (132):57–60.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Treatment of Calcific Tendinitis of the Gluteus Medius Muscle Using Ultrasound-Guided Barbotage Technique
- The Effect of One Leg Deadlift Exercise on the Muscle Activity of Lower Extremities according to the Weight Characteristics
- Sciatic Neuropathy after Intramuscular Injection at a Site Remote from the Nerve
- Thenar Compartment syndrome: A Case Report
- Calcific Tendinopathy of the Gluteus Medius Mimicking Lumbar Radicular Pain Successfully Treated With Barbotage: A Case Report
