Ann Rehabil Med.
2015 Oct;39(5):821-825. 10.5535/arm.2015.39.5.821.
Prolonged Motor Weakness With Syringomyelia in Japanese Encephalitis: A Case Study
- Affiliations
-
- 1Department of Rehabilitation Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. drpjh@catholic.ac.kr
- KMID: 2148214
- DOI: http://doi.org/10.5535/arm.2015.39.5.821
Abstract
- Japanese encephalitis (JE) shows characteristic brain lesions, including bilateral thalamus, midbrain, internal capsule, basal ganglia, and occasionally involves an anterior horn cell. We encountered a case of a 44-year-old man who initially presented with encephalitis, which was finally diagnosed as Japanese encephalomyelitis with syringomyelia. The patient showed severe motor weakness followed by delayed recovery of functional motor activities. Cervical magnetic resonance imaging showed syrinx formation at the C5 level suggesting myelitis, and abnormal electromyographic findings were noted. Clinicians should consider the possibility that the spinal cord may be involved; an example would be syringomyelia due to myelitis in a case of JE presenting with severe and prolonged motor weakness.
Keyword
MeSH Terms
Figure
-
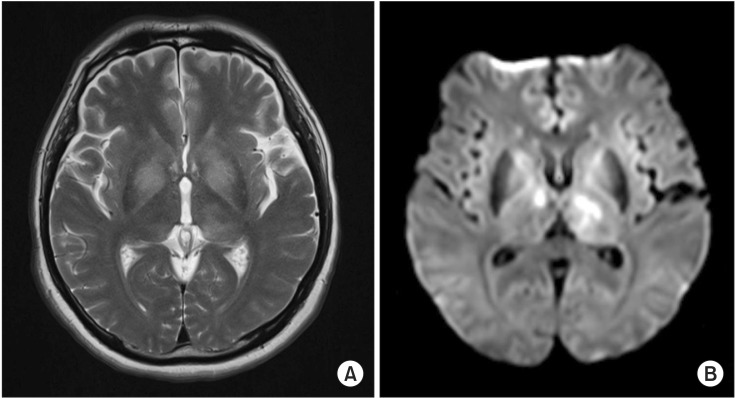
Fig. 1 Brain magnetic resonance imaging on the 28th day. (A) The axial T2-weighted image and (B) diffusion weighted image show characteristically high signal intensity in the bilateral thalamus and basal ganglia.
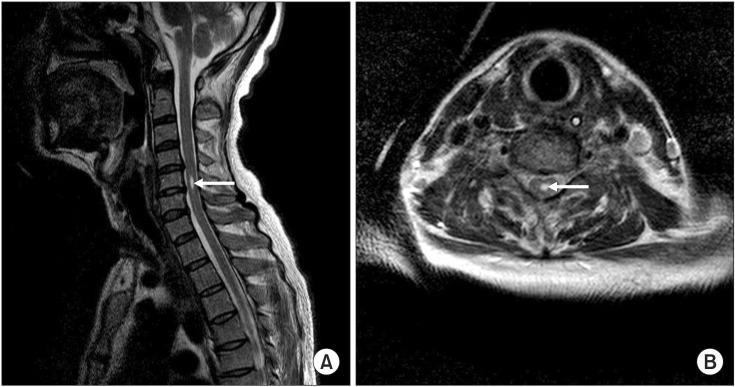
Fig. 2 Cervical magnetic resonance imaging on the 77th day. (A) Sagittal and (B) axial T2-weighted images show a cystic lesion with high signal intensity, suggesting syrinx formation (arrows) at the C5 level.

Fig. 3 Brain magnetic resonance imaging and diffusion tensor tractography (DTT) on the 87th day. (A) The DTT demonstrates the preserved integrity of both corticospinal tracts. (B) The diffusion weighted image shows the regression of high signal intensity in the bilateral thalamus and basal ganglia.
Reference
-
1. Solomon T, Dung NM, Kneen R, Gainsborough M, Vaughn DW, Khanh VT. Japanese encephalitis. J Neurol Neurosurg Psychiatry. 2000; 68:405–415. PMID: 10727474.2. Solomon T, Kneen R, Dung NM, Khanh VC, Thuy TT, Ha DQ, et al. Poliomyelitis-like illness due to Japanese encephalitis virus. Lancet. 1998; 351:1094–1097. PMID: 9660579.
Article3. Misra UK, Kalita J. Anterior horn cells are also involved in Japanese encephalitis. Acta Neurol Scand. 1997; 96:114–117. PMID: 9272188.
Article4. Verma R, Praharaj HN, Patil TB, Giri P. Acute transverse myelitis following Japanese encephalitis viral infection: an uncommon complication of a common disease. BMJ Case Rep. 2012; 9. 24. [Epub]. DOI: 10.1136/bcr-2012-007094.
Article5. Tzeng SS. Respiratory paralysis as a presenting symptom in Japanese encephalitis: a case report. Zhonghua Yi Xue Za Zhi (Taipei). 1989; 43:208–212. PMID: 2551472.6. Kumar S, Misra UK, Kalita J, Salwani V, Gupta RK, Gujral R. MRI in Japanese encephalitis. Neuroradiology. 1997; 39:180–184. PMID: 9106289.
Article7. Fischbein NJ, Dillon WP, Cobbs C, Weinstein PR. The "presyrinx" state: a reversible myelopathic condition that may precede syringomyelia. AJNR Am J Neuroradiol. 1999; 20:7–20. PMID: 9974051.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prolonged Limb and Respiratory Muscle Weakness Associated with Japanese Encephalitis Virus Infection: A Case Report
- Japanese Encephalitis in Korea, 2010: Case Reports and Epidemiology
- Haemagglutination inhibition antibodies of Japanese encephalitis virus to bats, Korea
- Syringomyelia & Syringobulbia in a Patient of Paraplegia Following Tuberculous Meningitis: Case report
- Japanese B Encephalitis with Favorable Recovery; Clinical Course, Brain Imaging, and Neuropsychological Findings
