Gender Difference in Bone Loss and Vascular Calcification Associated with Age
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Seoul St. Mary's Hospital, The Catholic University of Korea College of Medicne, Seoul, Korea. younhj@catholic.ac.kr
- 2Department of Radiology, Seoul St. Mary's Hospital, The Catholic University of Korea College of Medicne, Seoul, Korea.
- KMID: 2145500
- DOI: http://doi.org/10.4070/kcj.2013.43.7.453
Abstract
- BACKGROUND AND OBJECTIVES
It is widely known that both bone loss and vascular calcification are age-related processes. The purpose of this study was to investigate the relationship between coronary artery calcium (CAC) score or bone mineral density (BMD) with age and whether there is a gender difference factoring in the two conditions among healthy subjects.
SUBJECTS AND METHODS
Between March 2009 and August 2011, participants included 1727 subjects (mean age: 55+/-10 years, M : F=914 : 813) with routine health check-ups. After being categorized into three groups (normal, osteopenia, and osteoporosis) according to the World Health Organization (WHO) diagnostic classification, we estimated BMD by dual energy X-ray absorptiometry (DEXA) and CAC score by dual-source CT (DSCT).
RESULTS
There was a significant gender difference among the risk factors, including total-lumbar spine (1.213+/-0.176 g/cm2 : 1.087+/-0.168 g/cm2, p<0.001) and femur (1.024+/-0.131 g/cm2 : 0.910+/-0.127 g/cm2, p<0.001) in BMD by DEXA, and CAC score (68+/-227 : 27+/-116, p<0.001) in coronary artery calcification by DSCT. Age in male [odds ratio (OR): 1.138 {95% confidence interval (CI): 1.088-1.190}, p<0.001] and menopause in female subjects {OR: 12.370 (95% CI: 3.120-49.047), p<0.001} were, respectively, independently associated with osteopenia.
CONCLUSION
Although our results do not demonstrate a direct association between CAC score and BMD in both genders, there is a gender difference of CAC score in normal and osteopenia groups according to the WHO diagnostic classification. Additionally, we suggest that more specific therapeutic strategies be considered during any early bone loss period, especially in female subjects.
Keyword
MeSH Terms
Figure
-
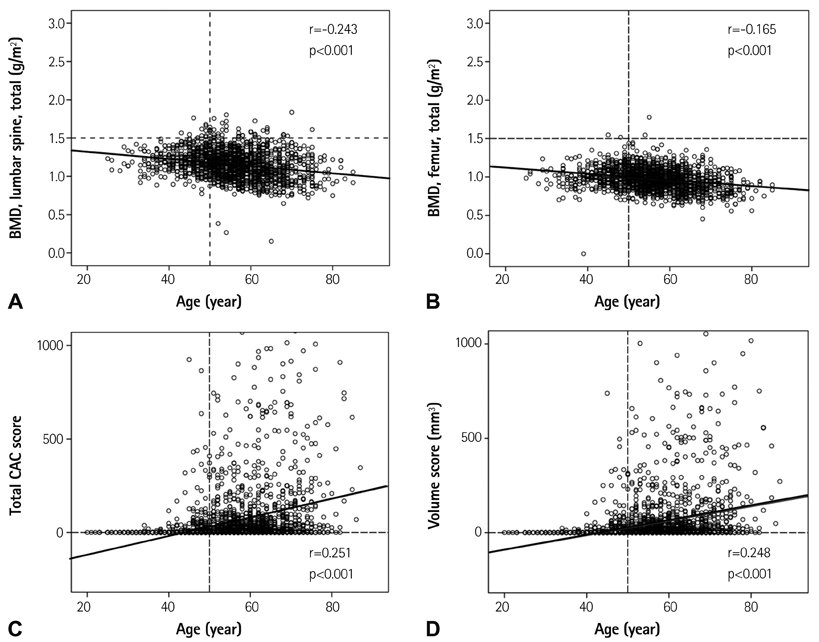
Fig. 1 Association with age in bone loss (A and B) and vascular calcification (C and D). BMD: bone mineral density, CAC: coronary artery calcium.
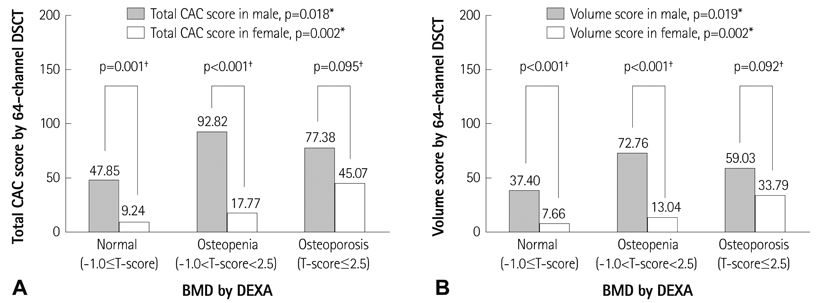
Fig. 2 Gender difference of each measurement for the three categorical groups according to the WHO diagnostic T-score criteria. Total CAC score (A) and volume score (B) by 64-channel DSCT. *The analysis for the three categorical groups according to the WHO diagnostic classification: normal, osteopenia and osteoporosis, was performed using analysis of variance test for continuous variables, †The analysis of gender difference was performed using an unpaired t-test for continuous variables. WHO: World Health Organization, CAC: coronary artery calcium, DSCT: dual source computed tomography, BMD: bone mineral density, DEXA: dual energy X-ray absorptiometry.
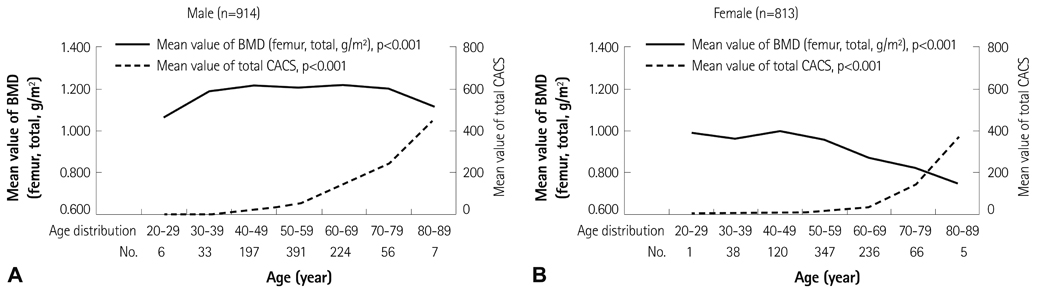
Fig. 3 Comparison of mean value of total BMD at the level of femur and total CAC score according to age distribution. The mean value of BMD at the level of femur decreases progressively, but total CAC score for vascular calcification increases sequentially through all ages in male subjects (A), while females aged 50 to 59 was a turning point for the abrupt decrease of BMD, but the sudden increase of total CAC score (B). p<0.05, the analysis for mean value of BMD and total CAC score according to age distribution was performed using analysis of variance test. BMD: bone mineral density, CAC: coronary artery calcium.
Reference
-
1. Kanis JA. WHO Study Group. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report. Osteoporos Int. 1994; 4:368–381.2. Kanis JA, Melton LJ 3rd, Christiansen C, Johnston CC, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res. 1994; 9:1137–1141.3. Farhat GN, Newman AB, Sutton-Tyrrell K, et al. The association of bone mineral density measures with incident cardiovascular disease in older adults. Osteoporos Int. 2007; 18:999–1008.4. Samelson EJ, Cupples LA, Broe KE, Hannan MT, O'Donnell CJ, Kiel DP. Vascular calcification in middle age and long-term risk of hip fracture: the Framingham Study. J Bone Miner Res. 2007; 22:1449–1454.5. Jørgensen L, Joakimsen O, Rosvold Berntsen GK, Heuch I, Jacobsen BK. Low bone mineral density is related to echogenic carotid artery plaques: a population-based study. Am J Epidemiol. 2004; 160:549–556.6. Frost ML, Grella R, Millasseau SC, et al. Relationship of calcification of atherosclerotic plaque and arterial stiffness to bone mineral density and osteoprotegerin in postmenopausal women referred for osteoporosis screening. Calcif Tissue Int. 2008; 83:112–120.7. Tankó LB, Christiansen C, Cox DA, Geiger MJ, McNabb MA, Cummings SR. Relationship between osteoporosis and cardiovascular disease in postmenopausal women. J Bone Miner Res. 2005; 20:1912–1920.8. Christian RC, Harrington S, Edwards WD, Oberg AL, Fitzpatrick LA. Estrogen status correlates with the calcium content of coronary atherosclerotic plaques in women. J Clin Endocrinol Metab. 2002; 87:1062–1067.9. Watson KE, Abrolat ML, Malone LL, et al. Active serum vitamin D levels are inversely correlated with coronary calcification. Circulation. 1997; 96:1755–1760.10. Parhami F, Morrow AD, Balucan J, et al. Lipid oxidation products have opposite effects on calcifying vascular cell and bone cell differentiation. A possible explanation for the paradox of arterial calcification in osteoporotic patients. Arterioscler Thromb Vasc Biol. 1997; 17:680–687.11. Lin T, Liu JC, Chang LY, Shen CW. Association between coronary artery calcification using low-dose MDCT coronary angiography and bone mineral density in middle-aged men and women. Osteoporos Int. 2011; 22:627–634.12. Choi SH, An JH, Lim S, et al. Lower bone mineral density is associated with higher coronary calcification and coronary plaque burdens by multidetector row coronary computed tomography in pre- and postmenopausal women. Clin Endocrinol (Oxf). 2009; 71:644–651.13. International Society for Clinical Densitometry Official Positions. updated 2007; cited 2008 July. Available from: http://www.iscd.org.14. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990; 15:827–832.15. Looker AC, Johnston CC Jr, Wahner HW, et al. Prevalence of low femoral bone density in older U.S. women from NHANES III. J Bone Miner Res. 1995; 10:796–802.16. Siris ES, Miller PD, Barrett-Connor E, et al. Identification and fracture outcomes of undiagnosed low bone mineral density in postmenopausal women: results from the National Osteoporosis Risk Assessment. JAMA. 2001; 286:2815–2822.17. Hernandez CJ, Beaupré GS, Carter DR. A theoretical analysis of the relative influences of peak BMD, age-related bone loss and menopause on the development of osteoporosis. Osteoporos Int. 2003; 14:843–847.18. Newman AB, Naydeck BL, Sutton-Tyrrell K, Feldman A, Edmundowicz D, Kuller LH. Coronary artery calcification in older adults to age 99: prevalence and risk factors. Circulation. 2001; 104:2679–2684.19. Yoon HC, Emerick AM, Hill JA, Gjertson DW, Goldin JG. Calcium begets calcium: progression of coronary artery calcification in asymptomatic subjects. Radiology. 2002; 224:236–241.20. Dawson-Hughes B, Tosteson AN, Melton LJ 3rd, et al. Implications of absolute fracture risk assessment for osteoporosis practice guidelines in the USA. Osteoporos Int. 2008; 19:449–458.21. Kanis JA, McCloskey EV, Johansson H, et al. Case finding for the management of osteoporosis with FRAX--assessment and intervention thresholds for the UK. Osteoporos Int. 2008; 19:1395–1408.22. Kim KI, Suh JW, Choi SY, et al. Is reduced bone mineral density independently associated with coronary artery calcification in subjects older than 50 years? J Bone Miner Metab. 2011; 29:369–376.23. Lee HT, Shin J, Lim YH, et al. The relationship between coronary artery calcification and bone mineral density in patients according to their metabolic syndrome status. Korean Circ J. 2011; 41:76–82.24. Bakhireva LN, Barrett-Connor EL, Laughlin GA, Kritz-Silverstein D. Differences in association of bone mineral density with coronary artery calcification in men and women: the Rancho Bernardo Study. Menopause. 2005; 12:691–698.25. Compston JE, Papapoulos SE, Blanchard F. Report on osteoporosis in the European Community: current status and recommendations for the future. Working Party from European Union Member States. Osteoporos Int. 1998; 8:531–534.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Vascular Calcification in Patients with Chronic Kidney Disease
- Clinical Implication of Vascular Calcification in Patients Undergoing Hemodialysis: The End or the Beginning of Disease
- Mechanisms of Vascular Calcification: The Pivotal Role of Pyruvate Dehydrogenase Kinase 4
- The Relation of Arterial Stiffness with Vascular Calcification and BMD in Chronic Kidney Disease
- The Effect of Severe Femoropopliteal Arterial Calcification on the Treatment Outcome of Femoropopliteal Intervention in Patients with Ischemic Tissue Loss
