Recurrent Acute Decompensated Heart Failure Owing to Severe Iron Deficiency Anemia Caused by Inappropriate Habitual Bloodletting
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, SMG-SNU Seoul Boramae Hospital, Seoul, Korea. shkimmd@snu.ac.kr
- 2Division of Hemato-Oncology, Department of Internal Medicine, SMG-SNU Seoul Boramae Hospital, Seoul, Korea.
- 3Department of Emergency Medicine and Cardiology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Internal Medicine, Hongik Hospital, Seoul, Korea.
- 5Department of Internal Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea.
- KMID: 2144456
- DOI: http://doi.org/10.4250/jcu.2015.23.4.253
Abstract
- A 68-year-old woman visited the emergency department twice with symptoms of acute heart failure including shortness of breath, general weakness, and abdominal distension. Laboratory findings showed extremely low level of serum hemoglobin at 1.4 g/dL. Echocardiographic examination demonstrated dilated left ventricular cavity with systolic dysfunction and moderate amount of pericardial effusion. In this patient, acute heart failure due to severe iron deficiency anemia was caused by inappropriate habitual bloodletting.
Keyword
MeSH Terms
Figure
-

Fig. 1 The 12-lead electrocardiogram showed normal sinus rhythm at a rate of 75 bpm, right axis deviation, and poor R-wave progression.
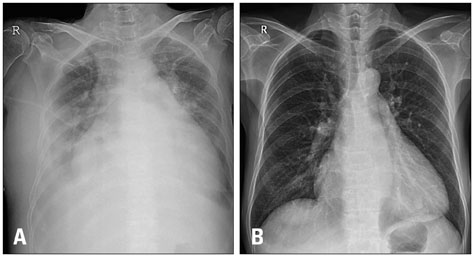
Fig. 2 The initial chest radiography demonstrated marked cardiomegaly and pulmonary edema with bilateral pleural effusion (A). After treatment of acute heart failure and anemia, follow-up radiograph showed a modest regression of cardiomegaly and resolution of pulmonary edema and pleural effusion (B).

Fig. 3 The transthoracic echocardiography revealed dilated left ventricular (LV) cavity (LV end-diastolic dimension = 63 mm) with mild LV dysfunction, eccentric LV hypertrophy, left atrial enlargement and moderate amount of pericardial effusion (A and B). Right sided chambers were also enlarged and moderate mitral regurgitation was observed (C and D).
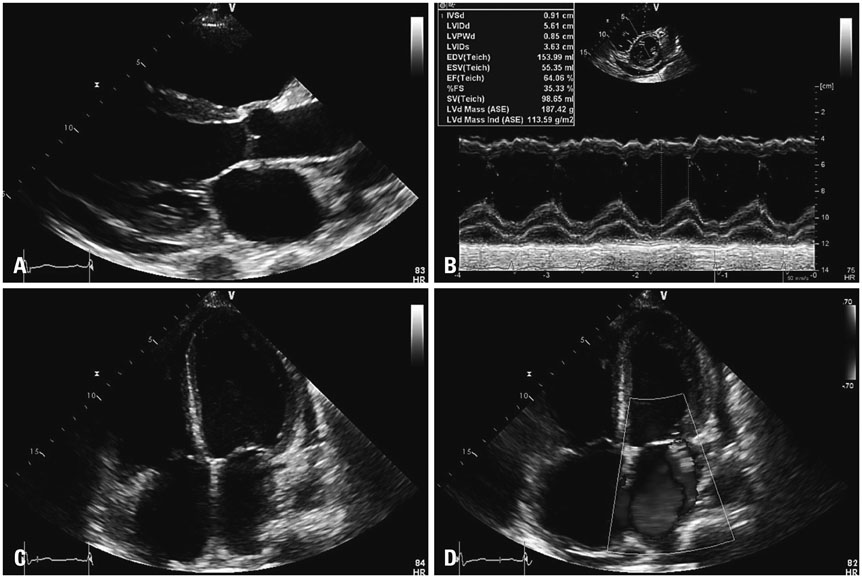
Fig. 4 The follow-up transthoracic echocardiography showed dilated left ventricular (LV) cavity (LV end-diastolic dimension = 56 mm) with low-normal LV function and small amount of pericardial effusion (A and B). Right sided chambers were still dilated and mitral regurgitation was reduced to mild degree (C and D).
Reference
-
1. Tang YD, Katz SD. The prevalence of anemia in chronic heart failure and its impact on the clinical outcomes. Heart Fail Rev. 2008; 13:387–392.2. Anand IS. Anemia and chronic heart failure implications and treatment options. J Am Coll Cardiol. 2008; 52:501–511.3. Mehta PA, Dubrey SW. High output heart failure. QJM. 2009; 102:235–241.4. Cohen-Solal A, Leclercq C, Deray G, Lasocki S, Zambrowski JJ, Mebazaa A, de Groote P, Damy T, Galinier M. Iron deficiency: an emerging therapeutic target in heart failure. Heart. 2014; 100:1414–1420.5. Anand IS, Chandrashekhar Y, Wander GS, Chawla LS. Endothelium-derived relaxing factor is important in mediating the high output state in chronic severe anemia. J Am Coll Cardiol. 1995; 25:1402–1407.6. Hegde N, Rich MW, Gayomali C. The cardiomyopathy of iron deficiency. Tex Heart Inst J. 2006; 33:340–344.7. Sohn IS, Jin ES, Cho JM, Kim CJ, Bae JH, Moon JY, Lee SH, Kim MJ. Bloodletting-induced cardiomyopathy: reversible cardiac hypertrophy in severe chronic anaemia from long-term bloodletting with cupping. Eur J Echocardiogr. 2008; 9:585–586.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Iron Deficiency Anemia due to Long-time Bloodletting Using Cupping
- Intravenous Iron Sucrose for Three Children with Iron Deficiency Anemia Failing to Respond to Oral Iron Therapy
- Molecular perspective of iron uptake, related diseases, and treatments
- H. pylori-associated Iron-Deficiency Anemia
- Iron Deficiency Anemia in Children and Adolescents
