Catheter Ablation of Atrial Fibrillation
- Affiliations
-
- 1Division of Cardiology, Korea University College of Medicine, Korea. yhkmd@unitel.co.kr
- KMID: 2137824
- DOI: http://doi.org/10.5124/jkma.2006.49.9.837
Abstract
- Atiarrhythmic drugs that are currently in use are not only frequently ineffective at eliminating atrial fibrillation (AF), but also life-threatening in some patients. However, the accumulating clinical experience along with the remarkable advancement in the technology has made the catheter ablation (CA) of AF more effective and safe. The application of circular mapping catheters that can identify pulmonary vein (PV) potentials (PVPs) within the PVs has allowed the effective guidance of the electrical isolation of the PVs from the left atrium (LA). The widespread utilization of 3-dimensional (D) mapping systems has facilitated the improvement of the outcomes after CA in patients with paroxysmal (PAF) and even chronic AF (CAF). Different strategies that are currently in use are as follows segmental ablation of each PV ostium guided by PVPs, pure anatomic approach of circumferential PV ablation (CPVA), CPVA with electrical isolation, complex fractionated atrial electrograms during AF guided ablation, and ablation of ganglionated plexuses, etc. The efficacy of each approach varies according to the investigators and subsets of AF. CPVA with electrical isolation is known to be more effective and is widely used. With further development of new energy sources of ablation and mapping systems, it is important to simplify, standardize, and shorten the procedures, which may enable the CA to become more effective, safe, and applicable to many different subsets of AF. CA of AF has evolved rapidly and has become accepted as one of the therapeutic modalities to cure AF.
Keyword
MeSH Terms
Figure
-
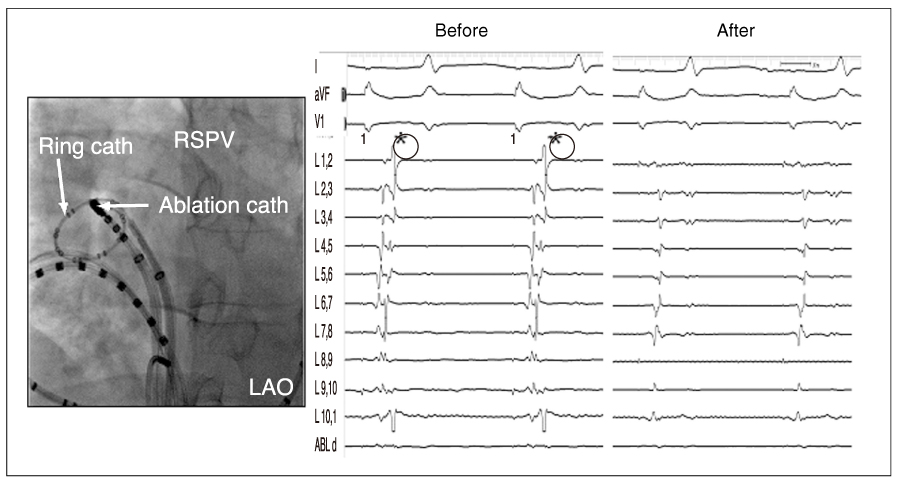
Figure 1 Pulmonary vein isolation confirmed by elimination of PVPs (*) PVP: pulmonary vein potential, RSPV: right superior pulmonary vein, LAO: left anterior oblique

Figure 2 Circumferential pulmonary vein ablation with isolation A) 3-Dimensional Mapping System Guided Circumferential Pulmonary Vein Ablation, B) Elimination of PVPs by Additional Ablation at the LA-PVJunction Showing PVPs After encircling of pulmonary veins (white circles in panel A), additional radiofrequency energy was delivered at the LA-PV junction (dark circles in panel A) to eliminate PVPs (*) as shown in panel B). LSPV: left superior pulmonary vein, LIPV: left inferior pulmonary vein, RSPV: right superior pulmonary vein, RIPV: right inferior pulmonary vein, LA-PV: left atrium-pulmonary vein, PVP: pulmonary vein potential

Figure 3 Recurrence rate of atrial fibrillation after catheter ablation in Korea University Medical Center PVA: pulmonary vein ablation. n indicates the accumulated number of patients
Reference
-
1. Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Corley SD, et al. Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002. 347:1825–1833.
Article2. Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Clementy J, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998. 339:659–666.
Article3. Rha SW, Kim YH, Park HN, Park SW, Shin SH, Kim EJ, et al. Initiation and Maintenance Mechanism of Atrial Fibrillation Assessed by 3-Dimensional Non-Contact Mapping System. Korean Circ J. 2004. 34:195–203.
Article4. Kim Y-H, Rha SW, Park SW, Park SM, Pak HN, Ro YM, et al. Wave frnt dynamics during atrial fibrillation with repetitive pulmonary vein tachycardia. Pacing Clin Electrophysiol. 2003. 26:1006(309).5. Haissaguerre M, Jais P, Shah DC, Garrigue S, Takahashi A, Clementy J, et al. Electrophysiological end point for catheter ablation of atrial fibrillation initiated from multiple pulmonary venous foci. Circulation. 2000. 101:1409–1417.
Article6. Marrouche NF, Dresing T, Cole C, Bash D, Saad E, Natale A, et al. Circular mapping and ablation of the pulmonary vein for treatment of atrial fibrillation: impact of different catheter technologies. J Am Coll Cardiol. 2002. 40:464–474.
Article7. Oral H, Knight BP, Tada H, Ozaydin M, Chugh A, Morady F, et al. Pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. Circulation. 2002. 105:1077–1081.
Article8. Lau CP, Tse HF, Ayers GM. Defibrillation-guided radiofrequency ablation of atrial fibrillation secondary to an atrial focus. J Am Coll Cardiol. 1999. 33:1217–1226.
Article9. Pappone C, Oreto G, Rosanio S, Vicedomini G, Tocchi M, Alfieri O, et al. Atrial electroanatomic remodeling after circumferential radiofrequency pulmonary vein ablation: efficacy of an anatomic approach in a large cohort of patients with atrial fibrillation. Circulation. 2001. 104:2539–2544.
Article10. Oral H, Scharf C, Chugh A, Hall B, Cheung P, Morady F, et al. Catheter ablation for paroxysmal atrial fibrillation: segmental pulmonary vein ostial ablation versus left atrial ablation. Circulation. 2003. 108:2355–2360.
Article11. Kottkamp H, Tanner H, Kobza R, Schirdewahn P, Dorszewski A, Hindricks G. et al. Time courses and quantitative analysis of atrial fibrillation episode number and duration after circular plus linear left atrial lesions: trigger elimination or substrate modification: early or delayed cure? J Am Coll Cardiol. 2004. 44:869–877.
Article12. Vasamreddy CR, Dalal D, Eldadah Z, Dickfeld T, Jayam VK, Calkins H, et al. Safety and efficacy of circumferential pulmonary vein catheter ablation of atrial fibrillation. Heart Rhythm. 2005. 2:42–48.
Article13. Ouyang F, Bansch D, Ernst S, Schaumann A, Hachiya H, Kuck KH. Complete isolation of left atrium surrounding the pulmonary veins: new insights from the double-Lasso technique in paroxysmal atrial fibrillation. Circulation. 2004. 110:2090–2096.
Article14. Nademanee K, McKenzie J, Kosar E, Schwab M, Sunsaneewitayakul B, Ngarmukos T, et al. A new approach for catheter ablation of atrial fibrillation: mapping of the electrophysiologic substrate. J Am Coll Cardiol. 2004. 43:2044–2053.
Article15. Nakagawa H, Scherlag BJ, Wu R, Po S, Lockwood D, Jackman WM, et al. Addition of selective ablation of autonomic ganglia to pulmonary vein antrum isolation for treatment of paroxysmal and persistent atrial fibrillation. Circulation. 2004. 110:III - 543.16. Scherlag BJ, Nakagawa H, Jackman WM, Yamanashi WS, Patterson E, Lazzara R, et al. Electrical stimulation to identify neural elements on the heart: their role in atrial fibrillation. J Interv Card Electrophysiol. 2005. 13:37–42.
Article17. Scherlag BJ, Yamanashi WS, Schauerte P, Scherlag M, Sun YX, Lazzara R, et al. Endovascular stimulation within the left pulmonary artery to induce slowing of heart rate and paroxysmal atrial fibrillation. Cardiovasc Res. 2002. 54:470–475.
Article18. Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Natale A, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation. JAMA. 2005. 293:2634–2640.
Article19. Hsu LF, Jais P, Sanders P, Garrigue S, Hocini M, Haissaguerre M. Catheter ablation for atrial fibrillation in congestive heart failure. N Engl J Med. 2004. 351:2373–2383.
Article20. Hocini M, Sanders P, Deisenhofer I, Jais P, Hsu LF, Haissaguerre M. Reverse remodeling of sinus node function after catheter ablation of atrial fibrillation in patients with prolonged sinus pauses. Circulation. 2003. 108:1172–1175.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
- Large Circular Ring Catheter Ablation Versus Anatomically Guided Ablation of Atrial Fibrillation: Back to the Future for Successful Catheter Ablation of Atrial Fibrillation?
- A Case of Chronic Radiodermatitis following Radiofrequency Catheter Ablation for Atrial Fibrillation
- The Mechanism of and Preventive Therapy for Stroke in Patients with Atrial Fibrillation
- Controlled Atrial Fibrillation after Pulmonary Vein Stenting
