Infective Endocarditis due to Streptococcus Agalactiae in Young and Immunocompetent Woman: A Case of Structurally Normal Valve Endocarditis Presented with Major Stroke
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Research Institute of Clinical Medicine, Chonbuk National University Medical School, Jeonju, Korea. whkim@jbnu.ac.kr
- KMID: 2135432
- DOI: http://doi.org/10.4250/jcu.2011.19.1.38
Abstract
- We describe here a 26-year-old woman who presented confusion and right hemiparesis due to embolic obstruction of left internal carotid artery and middle cerebral artery. Transthoracic echocardiography showed structurally normal mitral valve with hypermobile echogenic material suggesting vegetation. The vegetation was disappeared after antimicrobial treatment without surgery.
Keyword
MeSH Terms
Figure
-
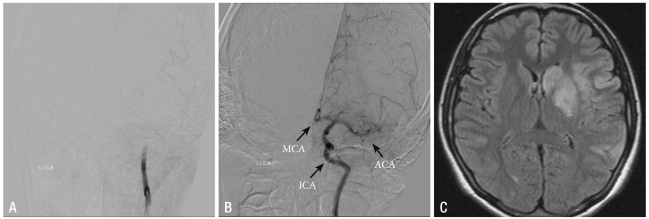
Fig. 1 Cerebral angiography shows complete thrombotic obstruction at the distal portion of left ICA (A). Final angiography after percutaneous thrombolysis shows good patency of left MCA, ACA and ICA (B). Brain MRI shows acute infarction in left MCA territory (circle) and focal hemorrhage in left lentiform nucleus (arrow) (C). ICA: internal carotid artery, MCA: middle cerebral artery, ACA: anterior cerebral artery, MRI: magnetic resonance imaging.
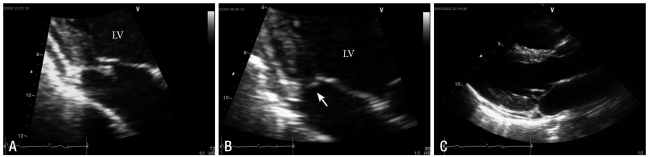
Fig. 2 Transthoracic echocardiography shows 0.8 × 0.5 cm-sized, echogenic and hypermobile mass on PMVL (A). Follow-up after antimicrobial therapy, echogenic mass was disappeared compared with previous study (B). Transthoracic echocardiography shows structurally normal MV during the end-systolic phase (C). PMVL: posterior mitral valve leaflet, MV: mitral valve.
Reference
-
1. Mylonakis E, Calderwood SB. Infective endocarditis in adults. N Engl J Med. 2001; 345:1318–1330. PMID: 11794152.2. Paterick TE, Paterick TJ, Nishimura RA, Steckelberg JM. Complexity and subtlety of infective endocarditis. Mayo Clin Proc. 2007; 82:615–621. PMID: 17493427.3. Beynon RP, Bahl VK, Prendergast BD. Infective endocarditis. BMJ. 2006; 333:334–339. PMID: 16902214.4. Hoen B. Epidemiology and antibiotic treatment of infective endocarditis: an update. Heart. 2006; 92:1694–1700. PMID: 17041124.5. Vilacosta I, Graupner C, San Roman JA, Sarria C, Ronderos R, Fernandez C, Mancini L, Sanz O, Sanmartin JV, Stoermann W. Risk of embolization after institution of antibiotic therapy for infective endocarditis. J Am Coll Cardiol. 2002; 39:1489–1495. PMID: 11985912.6. Baddour LM, Wilson WR, Bayer AS, Fowler VG Jr, Bolger AF, Levison ME, Ferrieri P, Gerber MA, Tani LY, Gewitz MH, Tong DC, Steckelberg JM, Baltimore RS, Shulman ST, Burns JC, Falace DA, Newburger JW, Pallasch TJ, Takahashi M, Taubert KA. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation. 2005; 111:e394–e434. PMID: 15956145.7. Park J, Choi SN, Kim HO, Jeong YG, Hwang JY, Kim JW, Bae IG. Two cases of infective endocarditis with multiple brain infarcts caused by Streptococcus agalactiae. Infect Chemother. 2006; 38:271–276.8. Lim TK, Kim SJ, Kim JH, Cho CB, Kim YJ, Kim KI, Lee SS. A case of infective endocarditis caused by Streptococcus agalactiae, in a patient with advanced gastric cancer. Korean J Med. 2009; 77:S209–S212.9. Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M, Bolger A, Cabell CH, Takahashi M, Baltimore RS, Newburger JW, Strom BL, Tani LY, Gerber M, Bonow RO, Pallasch T, Shulman ST, Rowley AH, Burns JC, Ferrieri P, Gardner T, Goff D, Durack DT. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007; 116:1736–1754. PMID: 17446442.10. Farley MM, Harvey RC, Stull T, Smith JD, Schuchat A, Wegner JD, Stephens DS. A population-based assessment of invasive disease due to group B streptococcus in nonpregnent adults. N Engl J Med. 1993; 328:1807–1811. PMID: 8502269.11. Ivanova Georgieva R, Carcia Lopez MV, Ruiz-morales J, Martinez-Marcos FJ, Lomas JM, Plata A, Noureddine M, Hidalgo-Tenorio C, Reguera JM, De la Torre Lima J, Galvez Aceval J, Marquez M, de Alarcon A. Streptococcus agalactiae left-sided infective endocarditis. Analysis of 27 cases from a multicentric cohort. J Infect. 2010; 61:54–59. PMID: 20417661.12. Sambola A, Miro JM, Tomas MP, Almirante B, Moreno-Torrico A, Gurgui M, Martinez E, Del Rio A, Azqueta M, Marco F, Gatell JM. Streptococcus agalactiae infective endocarditis: analysis of 30 cases and review of the literature 1962-1998. Clin Infect Dis. 2002; 34:1576–1584. PMID: 12032892.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Streptococcus Constellatus Community Acquired Pneumonia with Subsequent Isolated Pulmonic Valve Endocarditis and Abscess Formation in a Structurally Normal Heart
- A Case of Infective Endocarditis and Meningitis Caused by Streptococcus agalactiae
- A case of infective endocarditis caused by Streptococcus agalactiae, in a patient with advanced gastric cancer
- Infective Endocarditis due to Streptococcus pneumoniae
- A case of Libman-Sacks endocarditis confused with infective endocarditis
