Pulmonary Artery Angiosarcoma Confused with Acute Pulmonary Thromboembolism: Focusing on Clinical and Echocardiographic Features in the Differentiation of Two Categories
- Affiliations
-
- 1Department of Cardiology in Internal Medicine, Chungnam National University School of Medicine, Chungnam National University Hospital, Daejeon, Korea. jaehpark@cnu.ac.kr
- 2Department of Pathology, Chungnam National University School of Medicine, Chungnam National University Hospital, Daejeon, Korea.
- 3Department of Thoracic Surgery, Chungnam National University School of Medicine, Chungnam National University Hospital, Daejeon, Korea.
- KMID: 2135407
- DOI: http://doi.org/10.4250/jcu.2015.23.1.44
Abstract
- Although pulmonary artery angiosarcoma is rare, it can be misdiagnosed as pulmonary embolism because of its similar clinical and diagnostic features. The diagnosis is often delayed and the misdiagnosis brings unnecessary treatment. Because we made a wrong diagnosis of pulmonary artery angiosarcoma as an acute pulmonary embolism, we did thrombolytic therapy which could be dangerous to the patient. In this case report, we focused on the clinical and echocardiographic features of pulmonary artery angiosarcoma which can be used in differentiating the diagnosis from pulmonary embolism.
MeSH Terms
Figure
-
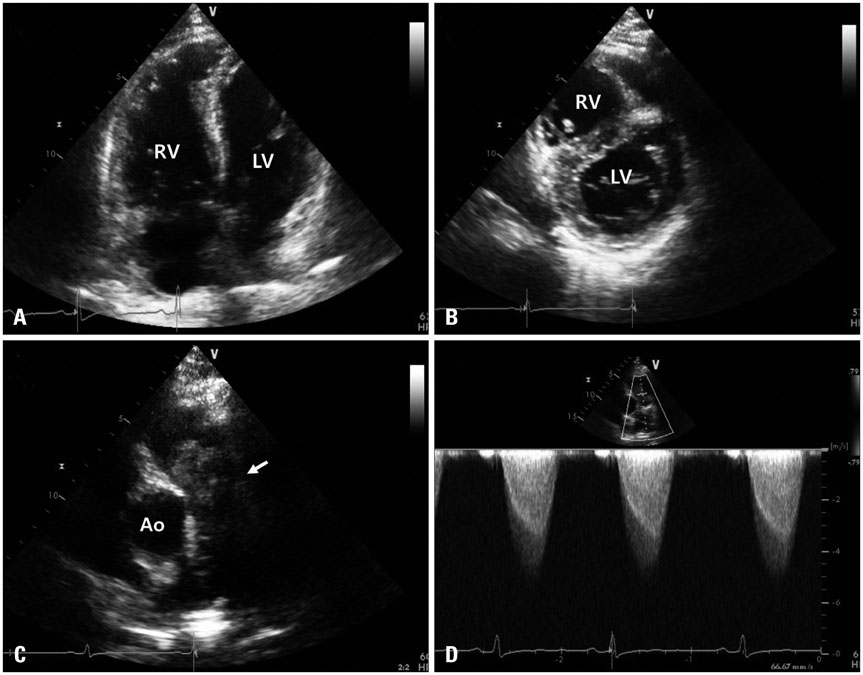
Fig. 1 Modified apical 4 chamber view shows dilated RV (A) and parasternal short axis view demonstrates D-shaped left ventricle indicating pressure overload of RV (B). Parasternal short axis view of the main pulmonary artery (MPA) reveals a mass lesion, about 50 × 30 mm sized, in the proximal part of the MPA with involvement of the pulmonary valves (arrow, C). The color Doppler imaging of the MPA shows flow acceleration during systole and the measured maximal velocity was about 4.6 m/sec (D). Ao: aorta, LV: left ventricle, RV: right ventricle.
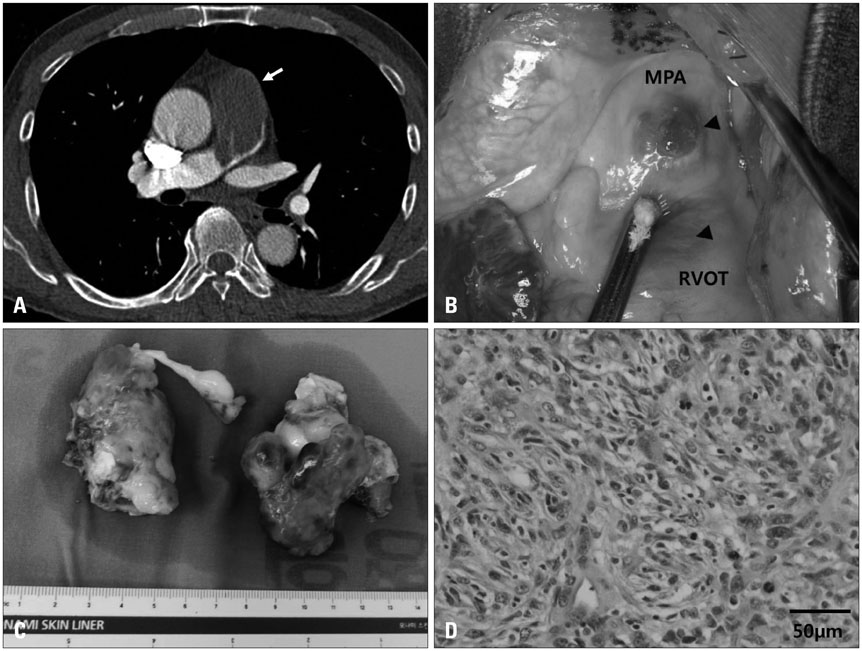
Fig. 2 Chest computerized tomographic scan demonstrates a large, about 58 × 31 mm sized, filling defect occupying the entire MPA with involvement of the pulmonary valves (arrow, A). Surgical finding shows the involvement of the anterior part of MPA and the RVOT (arrowheads, B). Resected tumor masses from the MPA and the RVOT demonstrates several hemorrhagic foci (C). It was divided into two separate parts during removal of the mass. The pathologic specimen demonstrated multiple pleomorphic spindle cells with mitotic figures indicating malignancy (hematoxylin and eosin stain, × 400, D). MPA: main pulmonary artery, RVOT: right ventricular outflow tract.
Reference
-
1. Nonomura A, Kurumaya H, Kono N, Nakanuma Y, Ohta G, Terahata S, Matsubara F, Matsuda T, Asaka T, Nishino T. Primary pulmonary artery sarcoma. Report of two autopsy cases studied by immunohistochemistry and electron microscopy, and review of 110 cases reported in the literature. Acta Pathol Jpn. 1988; 38:883–896.2. Anderson MB, Kriett JM, Kapelanski DP, Tarazi R, Jamieson SW. Primary pulmonary artery sarcoma: a report of six cases. Ann Thorac Surg. 1995; 59:1487–1490.3. Bleisch VR, Kraus FT. Polypoid sarcoma of the pulmonary trunk: analysis of the literature and report of a case with leptomeric organelles and ultrastructural features of rhabdomyosarcoma. Cancer. 1980; 46:314–324.4. Blackmon SH, Rice DC, Correa AM, Mehran R, Putnam JB, Smythe WR, Walkes JC, Walsh GL, Moran C, Singh H, Vaporciyan AA, Reardon M. Management of primary pulmonary artery sarcomas. Ann Thorac Surg. 2009; 87:977–984.5. Tschirch FT, Del Grande F, Marincek B, Huisman TA. Angiosarcoma of the pulmonary trunk mimicking pulmonary thromboembolic disease. A case report. Acta Radiol. 2003; 44:504–507.6. Huo L, Lai S, Gladish G, Czerniak BA, Moran CA. Pulmonary artery angiosarcoma: a clinicopathologic and radiological correlation. Ann Diagn Pathol. 2005; 9:209–214.7. Cox JE, Chiles C, Aquino SL, Savage P, Oaks T. Pulmonary artery sarcomas: a review of clinical and radiologic features. J Comput Assist Tomogr. 1997; 21:750–755.8. Wittlich N, Erbel R, Eichler A, Schuster S, Jakob H, Iversen S, Oelert H, Meyer J. Detection of central pulmonary artery thromboemboli by transesophageal echocardiography in patients with severe pulmonary embolism. J Am Soc Echocardiogr. 1992; 5:515–524.9. Oser RF, Zuckerman DA, Gutierrez FR, Brink JA. Anatomic distribution of pulmonary emboli at pulmonary angiography: implications for cross-sectional imaging. Radiology. 1996; 199:31–35.10. Yi CA, Lee KS, Choe YH, Han D, Kwon OJ, Kim S. Computed tomography in pulmonary artery sarcoma: distinguishing features from pulmonary embolic disease. J Comput Assist Tomogr. 2004; 28:34–39.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Artery Intimal Sarcoma Involving the Peripheral Pulmonary Artery, Initially Misdiagnosed as Pulmonary Artery Thromboembolism and Vasculitis: A Case Report
- Thromboendarterectomy of Chronic Pulmonary Thromboembolism: A Case Report
- Surgical Treatment of Pulmonary Artery Sarcoma: One case report
- Pulmonary Artery Intimal Sarcoma with Lung Metastasis
- Differential Imaging Features of Pulmonary Artery Dissection from Other Intraluminal Diseases of Pulmonary Artery: Two Cases Report
