Primary Hyperaparathyroidism due to Cystic Parathyroid Adenoma not Detected on 99mTc-Sestamibi Scan
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea. csshin@snu.ac.kr
- 2Department of Pathology, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Otorhinolaryngology, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2134824
- DOI: http://doi.org/10.3803/EnM.2012.27.1.83
Abstract
- Parathyroid cysts, which can be divided into functional and non-functional cysts, are rare causes of primary hyperparathyroidism. A technetium-99m-methoxyisobutylisonitrile (99mTc-sestamibi) parathyroid scan is a sensitive diagnostic tool for the localization, although it sometimes shows a false-negative result. Here we report a case of presumed cystic parathyroid adenoma based on clinical findings and analysis of cystic fluid with negative findings in a parathyroid scan. A 44-year-old male patient visited the hospital due to leg pain and compressive symptoms (dysphagia, hoarseness) that had started 4-5 months before. His serum calcium level was 14.4 mg/dL and his intact parathyroid hormone (iPTH) had increased to 478.1 pg/mL. On neck computed tomography, a cystic nodule measuring 6.2 cm was detected in the inferior part of the right thyroid gland. Sestamibi uptake for this nodule was not detected on 2-h delayed imaging, and fluorodeoxyglucose positron emission tomography showed only subtle uptake. Fine-needle aspiration was performed and intracystic iPTH had increased to 61,600 pg/mL. Focused parathyroidectomy guided by intraoperative iPTH monitoring led to successful enucleation of the right inferior parathyroid gland. A parathyroid adenoma was confirmed, and his laboratory results had normalized. This study shows that cystic parathyroid adenoma can sometimes be difficult to detect on a 99mTc-sestamibi parathyroid scan.
MeSH Terms
Figure
-
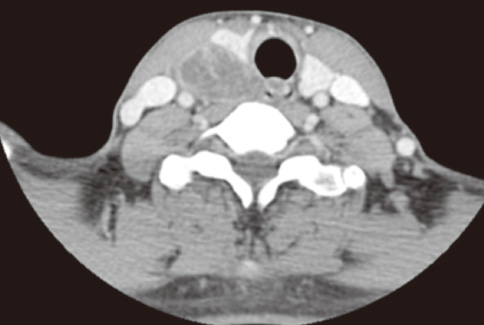
Fig. 1 Neck computed tomography shows a cystic lesion that measured 6.2 × 3.8 × 2.7 cm on the inferior side of the right thyroid lobe.
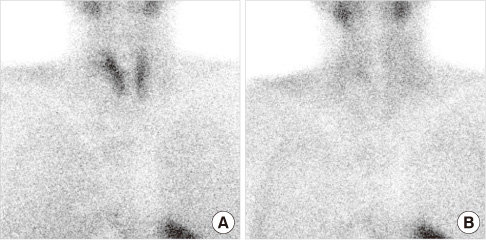
Fig. 2 After injection of 555 MBq (15 mCi) 99mTc-sestamibi, dual-phase scintigraphy was performed. Early (A, at 15 minute) and late (B, at 2.5 hour) images of the anterior neck were obtained using a low-energy high-resolution parallel-hole collimator. There was no 99mTc-sestamibi accumulation corresponding to the cystic lesion detected by neck computed tomography on either the early (A) or delayed (B) images.
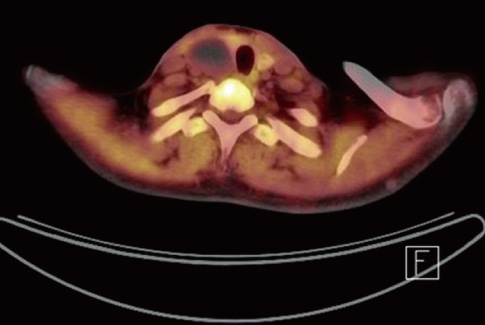
Fig. 3 Fluorodeoxyglucose positron emission tomography showed subtle uptake on the lower lobe of right thyroid gland.
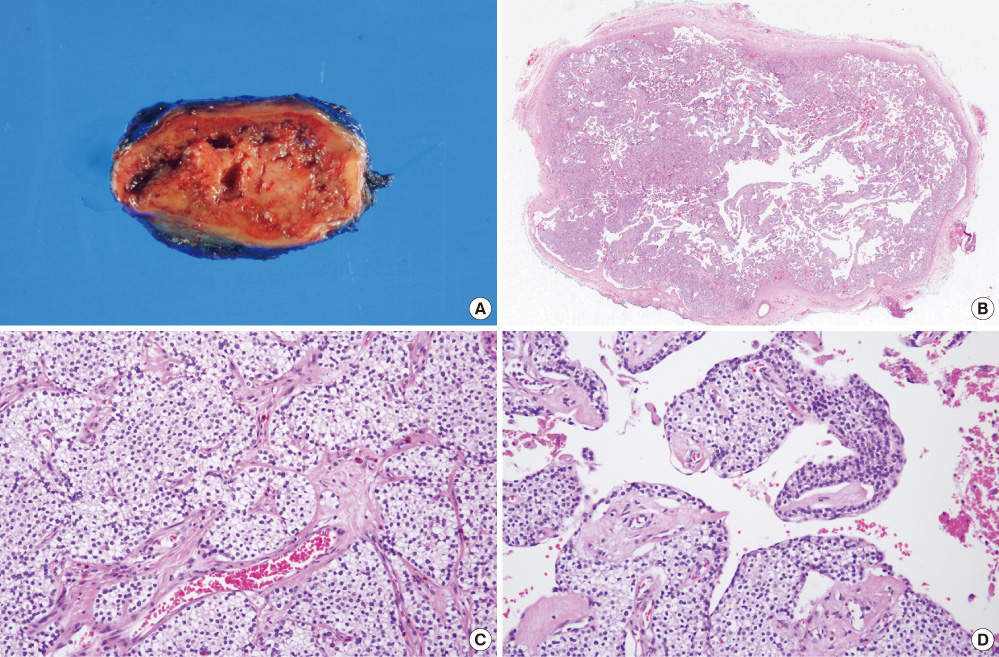
Fig. 4 Gross and microscopic findings of enucleated parathyroid adenoma. A. The tumor was encapsulated and cut surface showed brown color and cystic change. B. Low power view of parathyroid gland showing solid and cystic area (H&E stain, × 0.5). C. The solid area of tumor was showed hypercellular chief cells and well-vascularized (H&E stain, × 200). D. The cystic area of tumor showed vacant cavity with hemorrhage (H&E stain, × 200).
Reference
-
1. Rose DM, Wood TF, Van Herle AJ, Cohan P, Singer FR, Giuliano AE. Long-term management and outcome of parathyroidectomy for sporadic primary multiple-gland disease. Arch Surg. 2001. 136:621–626.2. Udelsman R. Six hundred fifty-six consecutive explorations for primary hyperparathyroidism. Ann Surg. 2002. 235:665–670.3. Armstrong J, Leteurtre E, Proye C. Intraparathyroid cyst: a tumour of branchial origin and a possible pitfall for targeted parathyroid surgery. ANZ J Surg. 2003. 73:1048–1051.4. Alabdulkarim Y, Nassif E. Sestamibi (99mTc) scan as a single localization modality in primary hyperparathyroidism and factors impacting its accuracy. Indian J Nucl Med. 2010. 25:6–9.5. Akbaba G, Berker D, Isik S, Aydin Y, Ciliz D, Peksoy I, Ozuguz U, Tutuncu YA, Guler S. A comparative study of preoperative imaging methods in patients with primary hyperparathyroidism: Us, Mibi, Spect and Mri. J Endocrinol Invest. 2011. In press.6. Ujiki MB, Nayar R, Sturgeon C, Angelos P. Parathyroid cyst: often mistaken for a thyroid cyst. World J Surg. 2007. 31:60–64.7. Swanson TW, Chan SK, Jones SJ, Bugis S, Irvine R, Belzberg A, Levine D, Wiseman SM. Determinants of Tc-99m sestamibi SPECT scan sensitivity in primary hyperparathyroidism. Am J Surg. 2010. 199:614–620.8. Chiu B, Sturgeon C, Angelos P. What is the link between nonlocalizing sestamibi scans, multigland disease, and persistent hypercalcemia? A study of 401 consecutive patients undergoing parathyroidectomy. Surgery. 2006. 140:418–422.9. Calandra DB, Shah KH, Prinz RA, Sullivan H, Hofmann C, Oslapas R, Ernst K, Lawrence AM, Paloyan E. Parathyroid cysts: a report of eleven cases including two associated with hyperparathyroid crisis. Surgery. 1983. 94:887–892.10. Biertho LD, Kim C, Wu HS, Unger P, Inabnet WB. Relationship between sestamibi uptake, parathyroid hormone assay, and nuclear morphology in primary hyperparathyroidism. J Am Coll Surg. 2004. 199:229–233.11. Bénard F, Lefebvre B, Beuvon F, Langlois MF, Bisson G. Rapid washout of technetium-99m-MIBI from a large parathyroid adenoma. J Nucl Med. 1995. 36:241–243.12. Siegel A, Alvarado M, Barth RJ Jr, Brady M, Lewis J. Parameters in the prediction of the sensitivity of parathyroid scanning. Clin Nucl Med. 2006. 31:679–682.13. Melloul M, Paz A, Koren R, Cytron S, Feinmesser R, Gal R. 99mTc-MIBI scintigraphy of parathyroid adenomas and its relation to tumour size and oxyphil cell abundance. Eur J Nucl Med. 2001. 28:209–213.14. Hetrakul N, Civelek AC, Stagg CA, Udelsman R. In vitro accumulation of technetium-99m-sestamibi in human parathyroid mitochondria. Surgery. 2001. 130:1011–1018.15. Sun SS, Shiau YC, Lin CC, Kao A, Lee CC. Correlation between P-glycoprotein (P-gp) expression in parathyroid and Tc-99m MIBI parathyroid image findings. Nucl Med Biol. 2001. 28:929–933.16. Jorna FH, Hollema H, Hendrikse HN, Bart J, Brouwers AH, Plukker JT. P-gp and MRP1 expression in parathyroid tumors related to histology, weight and (99m)Tc-sestamibi imaging results. Exp Clin Endocrinol Diabetes. 2009. 117:406–412.17. Carpentier A, Jeannotte S, Verreault J, Lefebvre B, Bisson G, Mongeau CJ, Maheux P. Preoperative localization of parathyroid lesions in hyperparathyroidism: relationship between technetium-99m-MIBI uptake and oxyphil cell content. J Nucl Med. 1998. 39:1441–1444.18. Fortson JK, Patel VG, Henderson VJ. Parathyroid cysts: a case report and review of the literature. Laryngoscope. 2001. 111:1726–1728.19. Neumann DR, Esselstyn CB, Maclntyre WJ, Go RT, Obuchowski NA, Chen EQ, Licata AA. Comparison of FDG-PET and sestamibi-SPECT in primary hyperparathyroidism. J Nucl Med. 1996. 37:1809–1815.20. Chen H, Pruhs Z, Starling JR, Mack E. Intraoperative parathyroid hormone testing improves cure rates in patients undergoing minimally invasive parathyroidectomy. Surgery. 2005. 138:583–587.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Primary Hyperparathyroidism Caused by Solitary Parathyroid Adenoma That was Not Detected by Both Ultrasonography and Sestamibi Scan
- Primary Hyperparathyroidism with Ectopic Parathyroid Adenoma Detected by Both 99mTc-MIBI SPECT and Contrast-Enhanced Neck CT
- Comparison of Ultrasonography and 99mTc-sestamibi Scan for Preoperative Localization of Parathyroid Adenoma
- A Case of Parathyroid Cancer with a Local Metastatic Focus Revealed by 99mTc-sestamibi scan
- Comparative Study of Preoperative Imaging Detection and Localization Test for Hyperparathyroidism
