Endoscopic Submucosal Dissection Using a Novel Versatile Knife: An Animal Feasibility Study (with Video)
- Affiliations
-
- 1Digestive Disease Center, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- 2Department of Pathology, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- 3Division of Gastroenterology and Hepatology, Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea. euschung@schmc.ac.kr
- 4Division of Gastroenterology, Department of Internal Medicine, Inha University School of Medicine, Incheon, Korea.
- KMID: 2134493
- DOI: http://doi.org/10.5946/ce.2014.47.6.544
Abstract
- BACKGROUND/AIMS
In order to reduce the procedure time and the number of accessory changes during endoscopic submucosal dissection (ESD), we developed a novel versatile knife, which has the combined advantages of several conventional knives. The aim of this study was to compare the efficacy, safety, and histological quality of ESD performed using this novel versatile knife and a combination of several conventional knives.
METHODS
This was an in vivo animal study comparing two different modalities of ESD in mini-pigs. Completion time of each resection was documented, and the resected specimens were retrieved and evaluated for completeness. To assess the quality control of the procedures and adverse events, detailed histopathological examinations were performed.
RESULTS
A total of 18 specimens were dissected by ESD safely and easily (nine specimens using the new versatile knife; nine specimens by mixing conventional knives). All resections were completed as en bloc resections. There was no significant difference in procedure time between the 2 modalities (456 seconds vs. 355 seconds, p=0.258) and cutting speed (1.983 mm2/sec vs. 1.57 mm2/sec, p=1.000). The rate of adverse events and histological quality did not statistically differ between the modalities.
CONCLUSIONS
ESD with a versatile knife appeared to be an easy, safe, and technically efficient method.
Figure
-
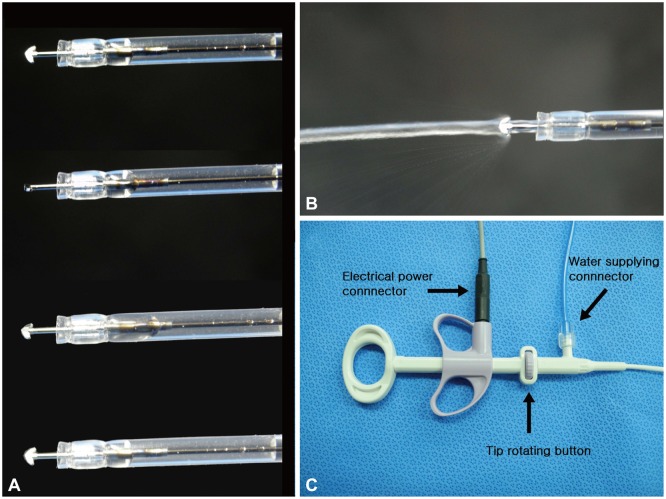
Fig. 1 The novel versatile knife (Optimos knife; Taewoong Medical) used in this study. (A) The Optimos knife has a 1.9-mm-wide and 2.5-mm-long anchor-shaped tip, which can be smoothly and fully rotated by controlling the dial on the handle of the knife. (B) The outer sheath can perform the water injection function. (C) The handle of the knife.
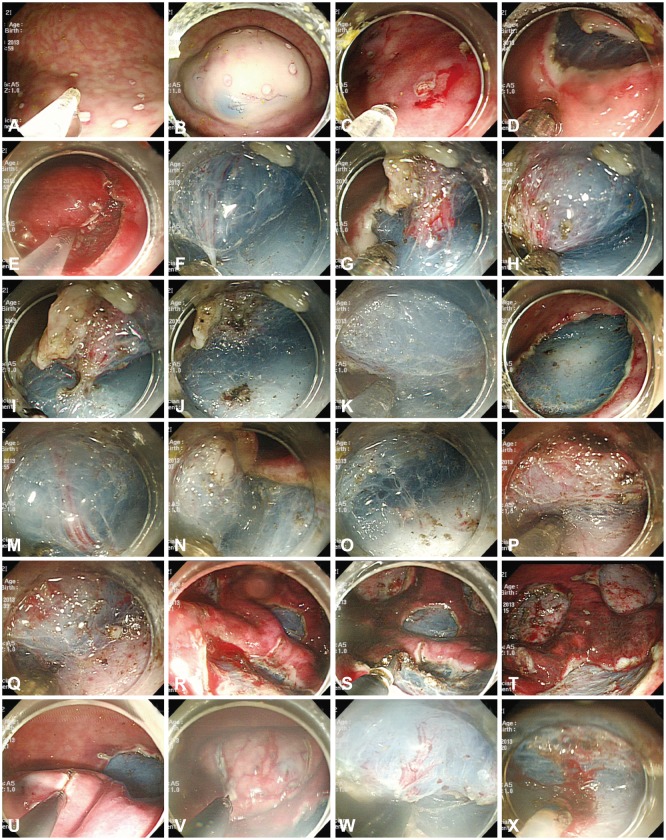
Fig. 2 Endoscopic submucosal dissection (ESD) procedures in the animal model. (A) Markings were made with the tip of the Optimos knife (Taewoong Medical) in the soft coagulation mode. (B) The mixed solution was repeatedly injected into the submucosal layer. (C-E) The tip of the Optimos knife was used to make the incision along the markings, using the endocut mode. (F-J) Submucosal dissection was carried out using the forced coagulation mode. The vessel was coagulated by the hooking method using the soft coagulation mode and cut using the endocut mode. (K, L) The distal remnant mucosal area was cut with the hooking method. (M-O) The knife can coagulate the small vessels of a ramified vascular network in a forced coagulation mode. (P, Q) The water injection system was used to keep enough fluid in the submucosa for continuous submucosal dissection. (R, S) The Coagrasper forceps were used to control major bleeding from large vessels, using the soft coagulation mode. (T) The post-ESD ulcers were shown to prevent bleeding afterward. (U-X) Three conventional knives (the IT-2, the Hook Knife, and the Dual knife) were used for ESD in the combination knives group.
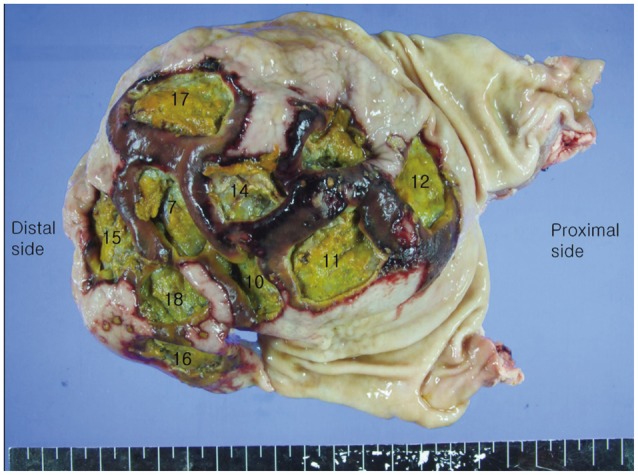
Fig. 3 Part of the stomach harvested from the second pig. Target lesions were centered on the greater curvature of the gastric body. The resected stomachs were incised along the lesser curvature to expose the interior, where no abnormality such as bleeding or perforation was found. The surrounding normal tissues were damaged and changed, but were not detected during endoscopic submucosal dissection. All numbers represent sequentially resected areas.
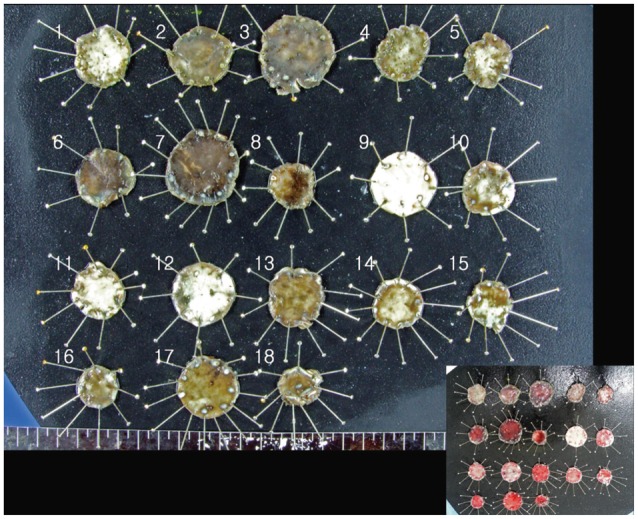
Fig. 4 Tissues from resected specimens pinned on a rubber board after formalin fixation. (Inset) Resected specimens just after the procedure.
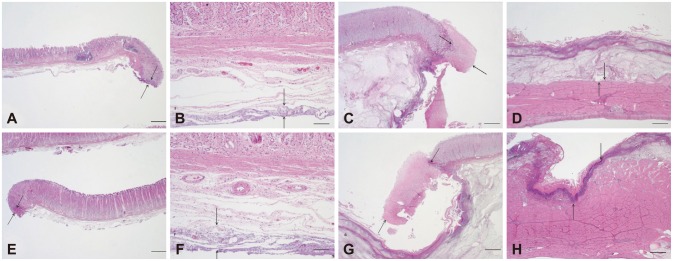
Fig. 5 Representative histological findings of endoscopic mucosal dissection (ESD) specimens and residual muscularis propria tissue from the Optimos knife group (A-D) and combination knives group (E-H; H&E stain). (A, B) ESD showing minimal injury to the lamina propria and submucosa in the Optimos knife group. (C, D) Residual bed tissue showing minimal injury to the lamina propria and muscularis propria in the Optimos knife group. (E, F) ESD showing minimal injury to the lamina propria and submucosa in the combination knives group. (G, H) Residual bed tissue showing marked injury in the lamina propria and muscularis propria in the combination knives group. Arrows represent the extent of injury. Scale bars represent 50 µm in (B) and (F) and 500 µm in the others.
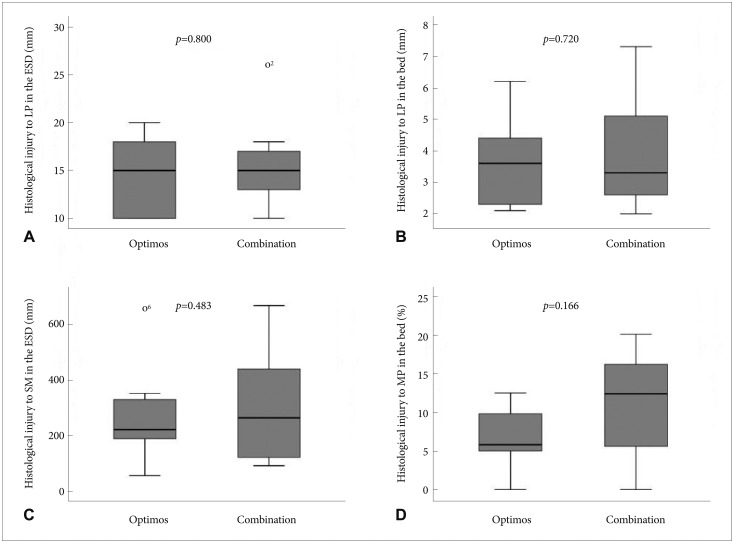
Fig. 6 Comparison of the levels of histological injury between the Optimos knife group and the combination knives group. (A) Extent of injury to the lamina propria in the dissected gastric specimens. (B) Extent of injury to the lamina propria in the remaining gastric bed tissue. (C) Depth of injury to the submucosa in the dissected gastric specimens. (D) Depth of injury to the MP in the remaining gastric bed tissue. LP, lamina propria; ESD, endoscopic mucosal dissection; SM, submucosa; MP, muscularis propria.
Reference
-
1. Ono H, Kondo H, Gotoda T, et al. Endoscopic mucosal resection for treatment of early gastric cancer. Gut. 2001; 48:225–229. PMID: 11156645.
Article2. Ohkuwa M, Hosokawa K, Boku N, Ohtu A, Tajiri H, Yoshida S. New endoscopic treatment for intramucosal gastric tumors using an insulated-tip diathermic knife. Endoscopy. 2001; 33:221–226. PMID: 11293753.
Article3. Yamamoto H, Kawata H, Sunada K, et al. Success rate of curative endoscopic mucosal resection with circumferential mucosal incision assisted by submucosal injection of sodium hyaluronate. Gastrointest Endosc. 2002; 56:507–512. PMID: 12297765.
Article4. Miyamoto S, Muto M, Hamamoto Y, et al. A new technique for endoscopic mucosal resection with an insulated-tip electrosurgical knife improves the completeness of resection of intramucosal gastric neoplasms. Gastrointest Endosc. 2002; 55:576–581. PMID: 11923778.
Article5. Chung IK, Lee JH, Lee SH, et al. Therapeutic outcomes in 1000 cases of endoscopic submucosal dissection for early gastric neoplasms: Korean ESD Study Group multicenter study. Gastrointest Endosc. 2009; 69:1228–1235. PMID: 19249769.
Article6. Yahagi N, Fujishiro M, Kakushima N, et al. Endoscopic submucosal dissection for early gastric cancer using the tip of an electrosurgical snare (thin type). Dig Endosc. 2004; 16:34–38.
Article7. Isomoto H, Shikuwa S, Yamaguchi N, et al. Endoscopic submucosal dissection for early gastric cancer: a large-scale feasibility study. Gut. 2009; 58:331–336. PMID: 19001058.
Article8. Watanabe K, Ogata S, Kawazoe S, et al. Clinical outcomes of EMR for gastric tumors: historical pilot evaluation between endoscopic submucosal dissection and conventional mucosal resection. Gastrointest Endosc. 2006; 63:776–782. PMID: 16650537.
Article9. Toyonaga T, Nishino E, Man IM, East JE, Azuma T. Principles of quality controlled endoscopic submucosal dissection with appropriate dissection level and high quality resected specimen. Clin Endosc. 2012; 45:362–374. PMID: 23251883.
Article10. Cao Y, Liao C, Tan A, Gao Y, Mo Z, Gao F. Meta-analysis of endoscopic submucosal dissection versus endoscopic mucosal resection for tumors of the gastrointestinal tract. Endoscopy. 2009; 41:751–757. PMID: 19693750.
Article11. Yamamoto H, Kita H. Endoscopic therapy of early gastric cancer. Best Pract Res Clin Gastroenterol. 2005; 19:909–926. PMID: 16338649.
Article12. Kakushima N, Fujishiro M. Endoscopic submucosal dissection for gastrointestinal neoplasms. World J Gastroenterol. 2008; 14:2962–2967. PMID: 18494043.
Article13. Conlin A, Kaltenbach T, Kusano C, Matsuda T, Oda I, Gotoda T. Endoscopic resection of gastrointestinal lesions: advancement in the application of endoscopic submucosal dissection. J Gastroenterol Hepatol. 2010; 25:1348–1357. PMID: 20659223.
Article14. Oyama T. Counter traction makes endoscopic submucosal dissection easier. Clin Endosc. 2012; 45:375–378. PMID: 23251884.
Article15. Neuhaus H. Endoscopic submucosal dissection in the upper gastrointestinal tract: present and future view of Europe. Dig Endosc. 2009; 21(Suppl 1):S4–S6. PMID: 19691732.
Article16. Toyonaga T, Man IM, Fujita T, et al. The performance of a novel ball-tipped Flush knife for endoscopic submucosal dissection: a case-control study. Aliment Pharmacol Ther. 2010; 32:908–915. PMID: 20839389.
Article17. Fujishiro M, Sugita N. Animal feasibility study of an innovated splash-needle for endoscopic submucosal dissection in the upper gastrointestinal tract. Dig Endosc. 2013; 25:7–12. PMID: 23286250.
Article18. Fukami N, Ryu CB, Said S, Weber Z, Chen YK. Prospective, randomized study of conventional versus HybridKnife endoscopic submucosal dissection methods for the esophagus: an animal study. Gastrointest Endosc. 2011; 73:1246–1253. PMID: 21316668.
Article19. Toyanaga T, Man IM, Ivanov D, et al. The results and limitations of endoscopic submucosal dissection for colorectal tumors. Acta Chir Iugosl. 2008; 55:17–23. PMID: 19069688.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison between a novel core knife and the conventional IT knife 2 for endoscopic submucosal dissection of gastric mucosal lesions
- Treatment of Early Gastric Cancer: Endoscopic Submucosal Dissection with LASER
- History and Development of Accessories for Endoscopic Submucosal Dissection
- Comparison of scissor-type knife to non-scissor-type knife for endoscopic submucosal dissection: a systematic review and meta-analysis
- Endoscopic Treatment of Subepithelial Tumors
