Brain Metastases of Papillary Thyroid Carcinoma with Horner's Syndrome
- Affiliations
-
- 1Department of Neurosurgery, College of Medicine, The Catholic University of Korea, Yeouido St. Mary's Hospital, Seoul, Korea. jwi@catholic.ac.kr
- KMID: 2134286
- DOI: http://doi.org/10.14791/btrt.2014.2.2.132
Abstract
- Papillary thyroid carcinoma (PTC) is the most common type of thyroid malignancy and has relatively favorable prognosis. Blood-borne metastases of PTC are very rare among the thyroid malignancies. Moreover a case of blood-borne central nervous system metastasized PTC with only unilateral Horner's syndrome, and without any abnormalities in laboratory or physical examinations has not been described before. A 53-year-old female patient had been managed in ophthalmologic clinic due to vague symptoms of right monocular blurred vision with eye dryness for 3 months, but showed no signs of improvement. So it was performed a magnetic resonance imaging and magnetic resonance angiography to evaluate the possibilities of cerebral lesion. And a left frontal mass was incidentally found, and the tumor turned out to be a PTC that had metastasized to brain, regional lymph node, cervical, thoracic spine, and lung. We describe a PTC with extraordinary initial symptoms that metastasized to an unusual site. We recommend that if a papillary thyroid tumor with unusual symptoms or at an advanced stage is found, further investigation should be performed for distant metastasis.
MeSH Terms
Figure
-
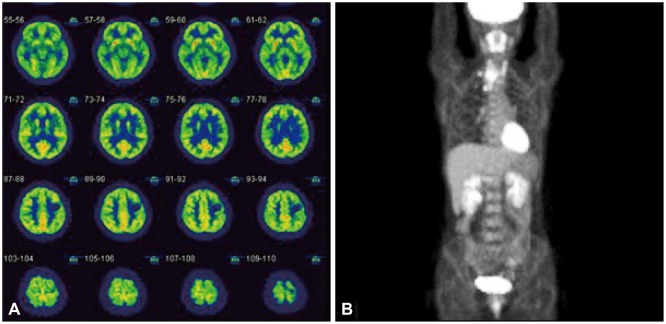
Fig. 1 Fluorodeoxyglucose-positron-emitting tomography image of (A) brain and (B) Torso. A cold spot is located on the left frontal lesion, a tumor mass uptakes glucose more than white matter, but surrounding normal gray matter more actively uptakes glucose. Papillary thyroid carcinoma is shown as hot uptake of cervical lesion in the Torso.
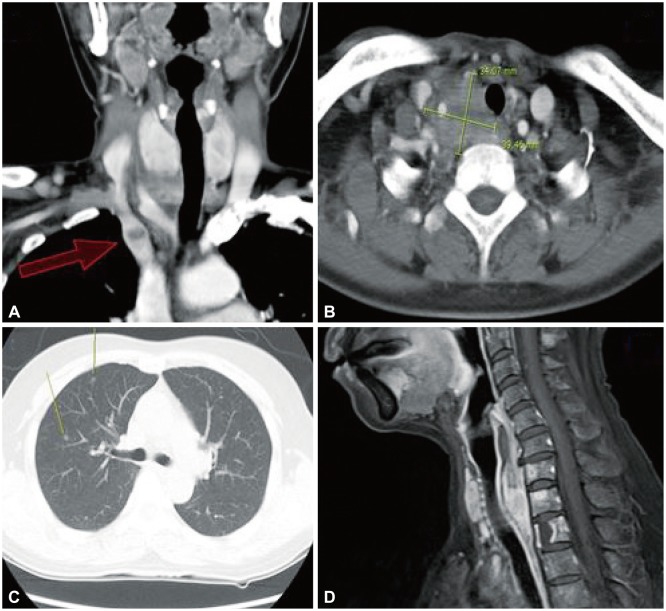
Fig. 2 The tumor growing toward mediastinum (red arrow) and retropharyngeal space and not which presenting goiter (A and D). The main mass located in deep cervical to lung apex lesion which encased major vessels and nerves, and deviated the trachea (B). Lung CT shows small nodular mass suspicious of metastasization from thyroid (C).
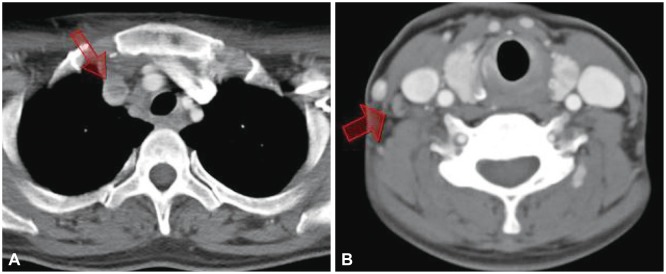
Fig. 3 Thyroid mass invaded into the vessel (arrow in A), with internal jugular venous thrombus (arrow in B) and cervical lymph node enlargement.
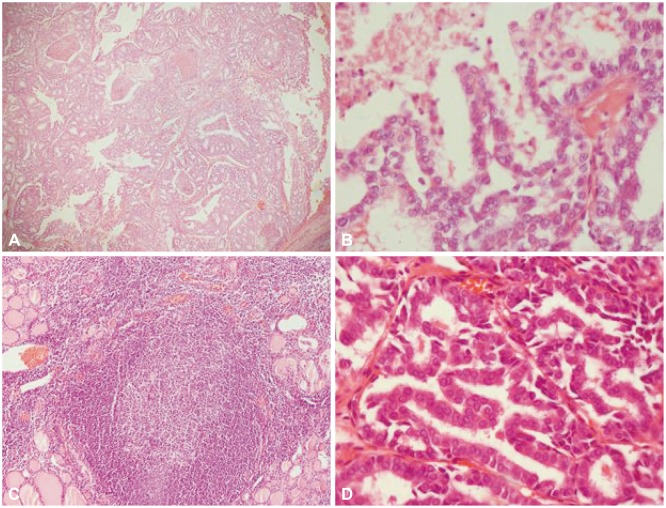
Fig. 4 Pathologic images of thyroid low magnification (A) and high magnification (B), which show irregular nuclear membrane with enlarged, grooved nucleus. Papillary thyroid carcinoma (PTC) coexisted with Hashimoto's thyroiditis (C). Metastasized cerebral tumor (D) showing same pathologic patterns as PTC. A and C: H&E, ×100. B and D: H&E, ×400.
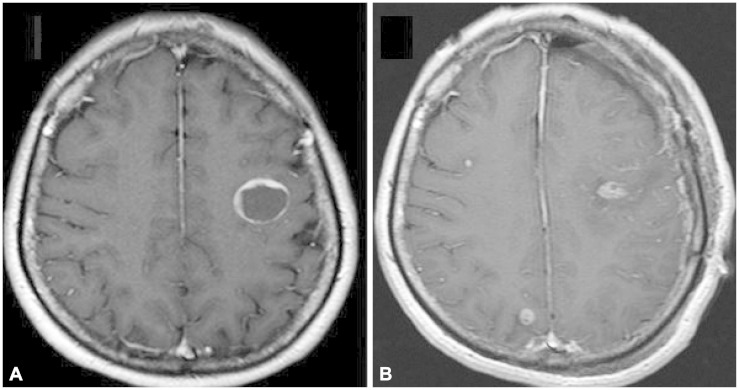
Fig. 5 Brain pre-operative enhanced MRI image (A). There is a single cystic mass in left frontal lobe. But in the post-operative enhanced MRI image (B) shows total removal of left frontal mass, but additional enhanced small mass were also found in right frontal and occipital lobe during the interval of 4 weeks.
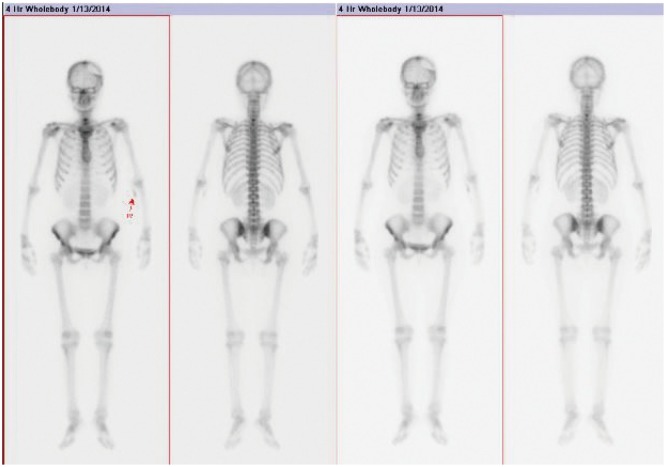
Fig. 6 Bone scan with Tc-99m-pertechnetate shows a defect in the left parietal bone, as sequel of the recent craniotomy surgery. There is a metastatic skeletal hot uptake lesion of lower cervical spine.
Reference
-
1. Miranda ER, Padrão EL, Silva BC, De Marco L, Sarquis MS. Papillary thyroid carcinoma with brain metastases: an unusual 10-year-survival case. Thyroid. 2010; 20:657–661. PMID: 20470207.
Article2. McCaffrey TV, Bergstralh EJ, Hay ID. Locally invasive papillary thyroid carcinoma: 1940-1990. Head Neck. 1994; 16:165–172. PMID: 8021137.
Article3. Gauden AJ, Gauden SJ. Multiple cerebral metastases as a primary presentation in papillary thyroid carcinoma. J Clin Neurosci. 2010; 17:379–380. PMID: 20074955.
Article4. Harding JL, Sywak MS, Sidhu S, Delbridge LW. Horner's syndrome in association with thyroid and parathyroid disease. ANZ J Surg. 2004; 74:442–445. PMID: 15191478.
Article5. Broome JT, Gauger PG, Miller BS, Doherty GM. Anaplastic thyroid cancer manifesting as new-onset Horner syndrome. Endocr Pract. 2009; 15:563–566. PMID: 19491063.
Article6. Tahmasebi FC, Farmer P, Powell SZ, et al. Brain metastases from papillary thyroid carcinomas. Virchows Arch. 2013; 462:473–480. PMID: 23532501.
Article7. Mazzaferri EL, Young RL, Oertel JE, Kemmerer WT, Page CP. Papillary thyroid carcinoma: the impact of therapy in 576 patients. Medicine (Baltimore). 1977; 56:171–196. PMID: 859443.8. Yamagami Y, Tori M, Sakaki M, Ohtake S, Nakahara M, Nakao K. Thyroid carcinoma with extensive tumor thrombus in the atrium. Gen Thorac Cardiovasc Surg. 2008; 56:555–558. PMID: 19002756.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Papillary Thyroid Cancer Arising in Lateral Aberrant Thyroid Presenting with Multiple Metastases
- Painful Horner syndrome after thyroidectomy: A case report
- Brain Metastasis from Papillary Carcinoma of the Thyroid
- Concurrent Medullay and Papillary Carcinoma of the Thyroid
- Occult Papillary Thyroid Carcinoma Presenting as a Metastatic Pleural Effusion
