Risk Factors Related to Hemorrhage Necessitating Renal Artery Embolization after Percutaneous Nephrostomy
- Affiliations
-
- 1Department of Radiology, Chonbuk National University Hospital and Medical School, Jeonju, Korea. ymhan@jbnu.ac.kr
- 2Research Institute of Clinical Medicine, Chonbuk National University Hospital and Medical School, Jeonju, Korea.
- 3Institute of Cardiovascular Research, Chonbuk National University Hospital and Medical School, Jeonju, Korea.
- KMID: 2130942
- DOI: http://doi.org/10.3348/jksr.2015.73.6.375
Abstract
- PURPOSE
To investigate risk factors related to severe bleeding necessitating renal artery embolization (RAE) after percutaneous nephrostomy (PCN).
MATERIALS AND METHODS
36 patients who underwent RAE from January 2005 to June 2014 were retrospectively reviewed. Among them, 10 patients underwent embolization because of severe bleeding after PCN (bleeding group). From 1762 patients who underwent PCN in the same period, we selected 21 patients who underwent PCN without bleeding after the procedure (non-bleeding group). We investigated possible related risk factors, such as the presence of underlying diseases, activated partial thromboplastin time (aPTT), prothrombin time (PT), platelet count, puncture site, procedure time, size of the kidney, distance from skin to renal cortex, maximum caliber of the indwelling catheter, parenchymal thickness, and grade of hydronephrosis. We used Fisher's exact test and independent t test for data analyses.
RESULTS
We classified hydronephrosis as either 'mild hydronephrosis,' or 'moderate or severe hydronephrosis.' The frequency of mild hydronephrosis was 80.0% (8/10) in the bleeding group and 33.3% (7/21) in the non-bleeding group (p = 0.023). There were no significant differences between the two groups in the incidence of underlying diseases. Similarly, other risk factors (PT, aPTT, platelet count, procedure time, distance from skin to renal cortex, maximum caliber of the indwelling catheter, kidney size, and parenhcymal thickness) also did not differ significantly between the two groups.
CONCLUSION
Mild hydronephrosis is a risk factor for severe bleeding necessitating RAE after PCN. Therefore, when performing PCN, careful attention should be paid to patients with mild hydronephrosis.
MeSH Terms
-
Catheters, Indwelling
Embolization, Therapeutic
Hemorrhage*
Humans
Hydronephrosis
Incidence
Kidney
Nephrostomy, Percutaneous*
Partial Thromboplastin Time
Platelet Count
Pregnenolone Carbonitrile
Prothrombin Time
Punctures
Renal Artery*
Retrospective Studies
Risk Factors*
Skin
Statistics as Topic
Pregnenolone Carbonitrile
Figure
-

Fig. 1 A 47-year-old woman with a left staghorn stone (arrow). A. The grade of hydronephrosis is 0 because there is no forniceal or calyceal dilatation. B. Contrast medium is administered intravenously to visualize the pelvocalyceal system. C. The patient had excessive hematuria 3 days after percutaneous nephrolithotomy. Pseudoaneurysm of interlobar artery (arrow) is detected on a renal arteriography.
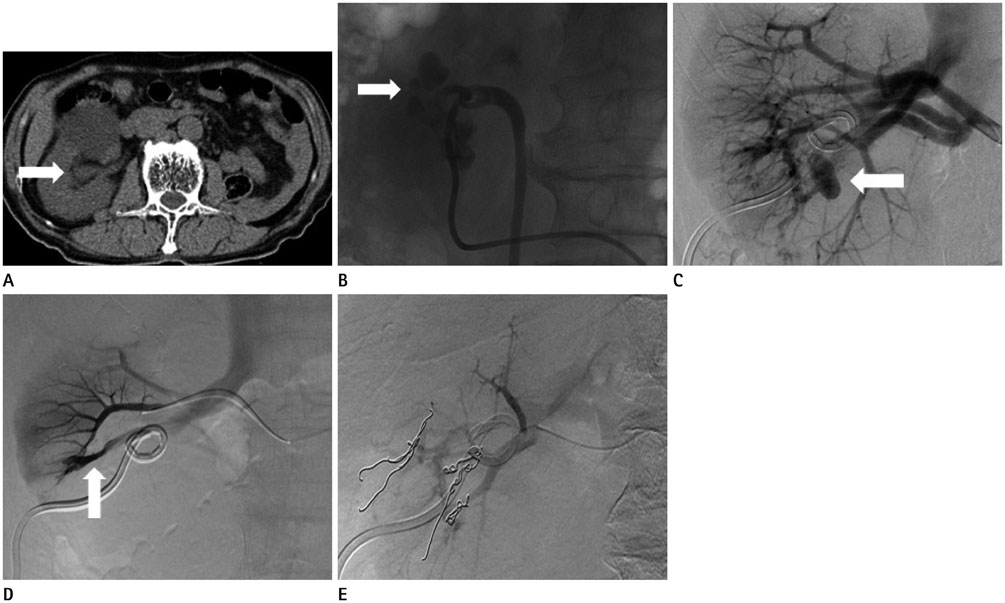
Fig. 2 An 83-year-old man with bladder cancer with invasion of the right distal ureter. A. The grade of hydronephrosis is 1 (arrow) because there is mild dilatation of the pelvis without dilatation of calyces. B. Successful percutaneous nephrostomy was performed in the mid to low pole. Dilated calyces (arrow) are filled with contrast media. C. Renal arteriography is performed because of persistent hematuria. Pseudoaneurysm (arrow) is detected in the low pole on the renal arteriography. D. Arteriovenous fistula (AVF) (arrow) is also discovered at selective angiogarphy. E. Psuedoaneurysm and AVF lesions are devascularized after coil embolization.
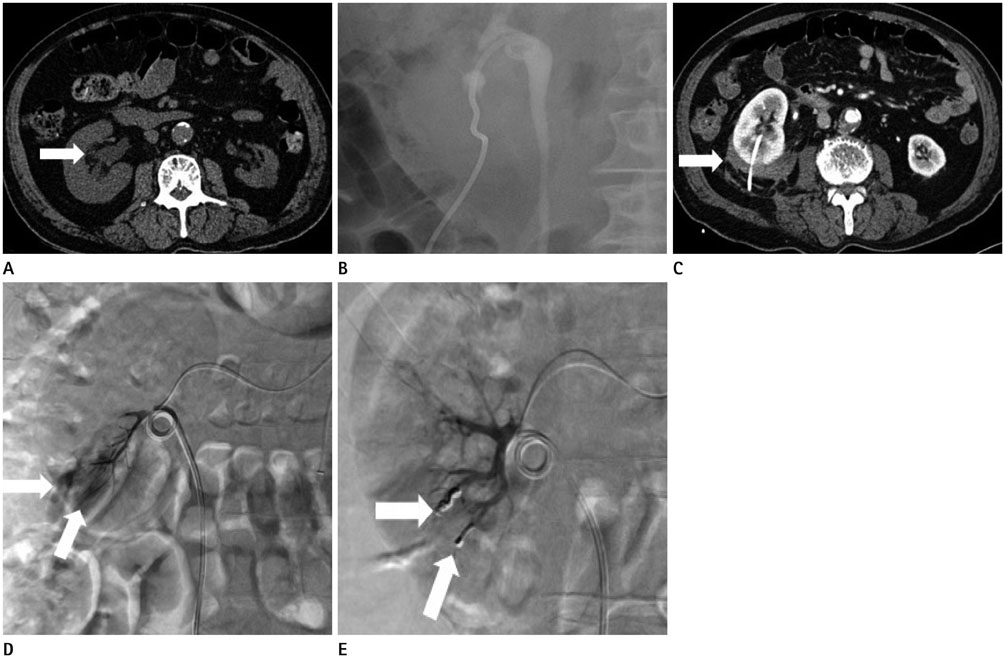
Fig. 3 A 78-year-old man with right distal ureteral stricture. The patient exhibited excessive hematuria after the procedure. A. The grade of hydronephrosis is 2 (arrow) because there is mild dilatation of the pelvis and calyces. B. Successful percutaneous nephrostomy was performed in the low pole. C. Hemorrhage in perinephric space of right kidney (arrow) is detected by abdominal CT following the procedure. D. Two arteriovenous fistulae of the interlobar artery (arrows) are present in the low pole of the right kidney. E. The feeding vessels are devascularized after coil embolization (arrows).
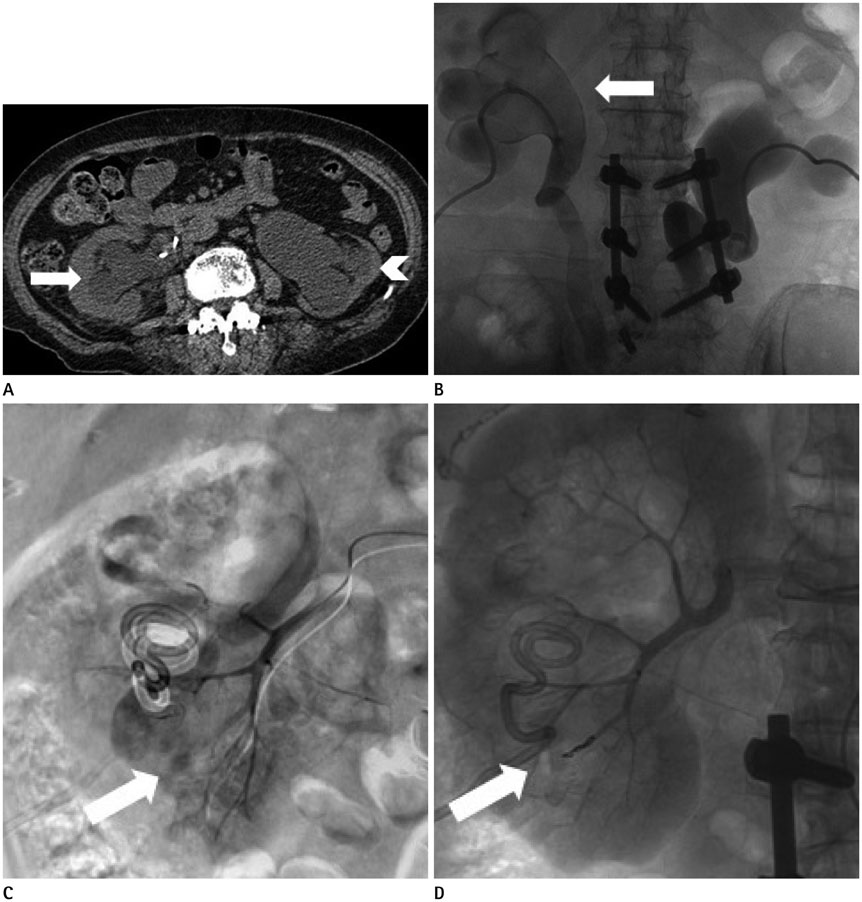
Fig. 4 A 69-year-old woman with cervical cancer given bilateral D-J stents for double-sided ureteral invasion. A. Malfunction of both D-J stents was suggested. The grade of hydronephrois is 3 in the right kidney (arrow) and 4 in the left kidney (arrowhead). B. After removal of both D-J stents with snares, percutaneous nephrostomy was performed successfully. A filling defect caused by hematoma is discovered in the right pelvocalyceal system (arrow). C. Upon renal arteriography, a pseudoaneurym of an interlobar artery (arrow) is discovered in the low pole of the right kidney. D. The feeding vessel is devascularized after coil embolization (arrow).
Reference
-
1. Cope C, Zeit RM. Pseudoaneurysms after nephrostomy. AJR Am J Roentgenol. 1982; 139:255–261.2. Potter SR, Chow GK, Jarrett TW. Percutaneous endoscopic management of urothelial tumors of the renal pelvis. Urology. 2001; 58:457–459.3. Ali SM, Mehmood K, Faiq SM, Ali B, Naqvi SA, Rizvi AU. Frequency of complications in image guided percutaneous nephrostomy. J Pak Med Assoc. 2013; 63:816–820.4. Lee WJ, Smith AD, Cubelli V, Badlani GH, Lewin B, Vernace F, et al. Complications of percutaneous nephrolithotomy. AJR Am J Roentgenol. 1987; 148:177–180.5. Stoller ML, Wolf JS Jr, St Lezin MA. Estimated blood loss and transfusion rates associated with percutaneous nephrolithotomy. J Urol. 1994; 152(6 Pt 1):1977–1981.6. Kessaris DN, Bellman GC, Pardalidis NP, Smith AG. Management of hemorrhage after percutaneous renal surgery. J Urol. 1995; 153(3 Pt 1):604–608.7. Sampaio FJ. Renal anatomy. Endourologic considerations. Urol Clin North Am. 2000; 27:585–607. vii8. Patterson DE, Segura JW, LeRoy AJ, Benson RC Jr, May G. The etiology and treatment of delayed bleeding following percutaneous lithotripsy. J Urol. 1985; 133:447–451.9. Gallucci M, Fortunato P, Schettini M, Vincenzoni A. Management of hemorrhage after percutaneous renal surgery. J Endourol. 1998; 12:509–512.10. Maleux G, Stockx L, Wilms G, Bogaert G, Marchal G. Postoperative retroperitoneal hemorrhage due to a bleeding ureteric artery: treatment by transcatheter embolization. Eur Radiol. 2001; 11:34–36.11. Zapzalka DM, Thompson HA, Borowsky SS, Coleman-Steenson CC, Mahowald ML, O'Connell KJ. Polyarteritis nodosa presenting as spontaneous bilateral perinephric hemorrhage: management with selective arterial embolization. J Urol. 2000; 164:1294–1295.12. Fernbach SK, Maizels M, Conway JJ. Ultrasound grading of hydronephrosis: introduction to the system used by the Society for Fetal Urology. Pediatr Radiol. 1993; 23:478–480.13. Konda R, Sakai K, Ota S, Abe Y, Hatakeyama T, Orikasa S. Ultrasound grade of hydronephrosis and severity of renal cortical damage on 99m technetium dimercaptosuccinic acid renal scan in infants with unilateral hydronephrosis during followup and after pyeloplasty. J Urol. 2002; 167:2159–2163.14. Kukreja R, Desai M, Patel S, Bapat S, Desai M. Factors affecting blood loss during percutaneous nephrolithotomy: prospective study. J Endourol. 2004; 18:715–722.15. Martin JH, Rosser CJ, Linebach RF, McCullough DL, Assimos DG. Are coagulation studies necessary before percutaneous nephrostomy? Tech Urol. 2000; 6:205–207.16. Kervancioglu S, Gelebek Yilmaz F, Erturhan S. Endovascular management of vascular complications after percutaneous nephrolithotomy. Vasa. 2014; 43:459–464.17. Gray RR, So CB, McLoughlin RF, Pugash RA, Saliken JC, Macklin NI. Outpatient percutaneous nephrostomy. Radiology. 1996; 198:85–88.18. Farrell TA, Hicks ME. A review of radiologically guided percutaneous nephrostomies in 303 patients. J Vasc Interv Radiol. 1997; 8:769–774.19. Dyer RB, Assimos DG, Regan JD. Update on interventional uroradiology. Urol Clin North Am. 1997; 24:623–652.20. Zagoria RJ, Dyer RB. Do's and don't's of percutaneous nephrostomy. Acad Radiol. 1999; 6:370–377.21. Dyer RB, Regan JD, Kavanagh PV, Khatod EG, Chen MY, Zagoria RJ. Percutaneous nephrostomy with extensions of the technique: step by step. Radiographics. 2002; 22:503–525.22. Michel MS, Trojan L, Rassweiler JJ. Complications in percutaneous nephrolithotomy. Eur Urol. 2007; 51:899–906. discussion 906.23. Sharma G, Sharma A. Determining the angle and depth of puncture for fluoroscopy-guided percutaneous renal access in the prone position. Indian J Urol. 2015; 31:38–41.24. Alyami FA, Skinner TA, Norman RW. Impact of body mass index on clinical outcomes associated with percutaneous nephrolithotomy. Can Urol Assoc J. 2013; 7:E197–E201.25. Torrecilla Ortiz C, Meza Martínez AI, Vicens Morton AJ, Vila Reyes H, Colom Feixas S, Suarez Novo JF, et al. Obesity in percutaneous nephrolithotomy. Is body mass index really important? Urology. 2014; 84:538–543.26. Smith AD. Percutaneous punctures--is this the endourologist's turf? J Urol. 1994; 152(6 Pt 1):1982–1983.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Glued Angiocatheter: A Rare Complication of Intrarenal Pseudoaneurysm Glue Angioembolization
- A case of nephro-colo-cutaneous fistula after percutaneous nephrostomy
- Renal Pseudoaneurysm after Percutaneous Nephrolithotomy
- Percutaneous Nephrostomy: Experience in 101 Cases
- Comparison of Renal Hemorrahge According to Technique of Percutaneous Tract Dilation in Percutaneous Nephrolithotomy
