Yonsei Med J.
2014 Jul;55(4):1063-1071. 10.3349/ymj.2014.55.4.1063.
Combined Muscle Motor and Somatosensory Evoked Potentials for Intramedullary Spinal Cord Tumour Surgery
- Affiliations
-
- 1Department of Neurosurgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. scrhim@amc.seoul.kr
- 2Department of Neurosurgery, Spine Center, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- 3Department of Neurology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2130834
- DOI: http://doi.org/10.3349/ymj.2014.55.4.1063
Abstract
- PURPOSE
To evaluate whether intraoperative neurophysiologic monitoring (IONM) with combined muscle motor evoked potentials (mMEPs) and somatosensory evoked potentials is useful for more aggressive and safe resection in intramedullary spinal cord tumour (IMSCT) surgery.
MATERIALS AND METHODS
We reviewed data from consecutive patients who underwent surgery for IMSCT between 1998 and April 2012. The patients were divided into two groups based on whether or not IONM was applied. In the monitored group, the procedures were performed under IONM using 75% muscle amplitude decline weaning criteria. The control group was comprised of patients who underwent IMSCT surgery without IONM. The primary outcome was the rate of gross total excision of the tumour on magnetic resonance imaging at one week after surgery. The secondary outcome was the neurologic outcome based on the McCormick Grade scale.
RESULTS
The two groups had similar demographics. The total gross removal tended to increase when intraoperative neurophysiologic monitoring was used, but this tendency did not reach statistical significance (76% versus 58%; univariate analysis, p=0.049; multivariate regression model, p=0.119). The serial McCormick scale score was similar between the two groups (based on repeated measure ANOVA).
CONCLUSION
Our study evaluated combined IONM of trans-cranial electrical (Tce)-mMEPs and SEPs for IMSCT. During IMSCT surgery, combined Tce-mMEPs and SEPs using 75% muscle amplitude weaning criteria did not result in significant improvement in the rate of gross total excision of the tumour or neurologic outcome.
MeSH Terms
Figure
-

Fig. 1 Comparison two groups with McCormickscale score. POD, post operative day.
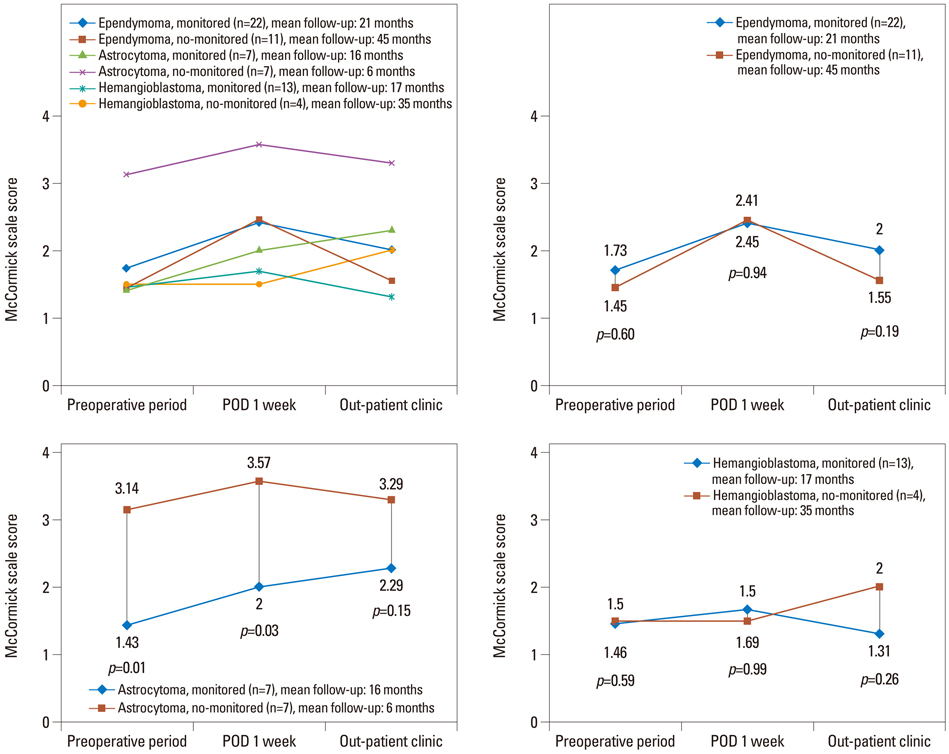
Fig. 2 Repeated measured ANOVA comparing effect of monitoring according IMSCT histology. POD, post operative day; IMSCT, intramedullary spinal cord tumour; ANOVA, analysis of variance.
Cited by 1 articles
-
Monitoring of Motor and Somatosensory Evoked Potentials During Spine Surgery: Intraoperative Changes and Postoperative Outcomes
Shin Hye Chang, Yoon Ghil Park, Dae Hyun Kim, Seo Yeon Yoon
Ann Rehabil Med. 2016;40(3):470-480. doi: 10.5535/arm.2016.40.3.470.
Reference
-
1. Cristante L, Herrmann HD. Surgical management of intramedullary spinal cord tumors: functional outcome and sources of morbidity. Neurosurgery. 1994; 35:69–74.2. McCormick PC, Torres R, Post KD, Stein BM. Intramedullary ependymoma of the spinal cord. J Neurosurg. 1990; 72:523–532.
Article3. Hoshimaru M, Koyama T, Hashimoto N, Kikuchi H. Results of microsurgical treatment for intramedullary spinal cord ependymomas: analysis of 36 cases. Neurosurgery. 1999; 44:264–269.
Article4. Constantini S, Miller DC, Allen JC, Rorke LB, Freed D, Epstein FJ. Radical excision of intramedullary spinal cord tumors: surgical morbidity and long-term follow-up evaluation in 164 children and young adults. J Neurosurg. 2000; 93:2 Suppl. 183–193.
Article5. Epstein FJ, Farmer JP, Freed D. Adult intramedullary spinal cord ependymomas: the result of surgery in 38 patients. J Neurosurg. 1993; 79:204–209.
Article6. Guidetti B, Mercuri S, Vagnozzi R. Long-term results of the surgical treatment of 129 intramedullary spinal gliomas. J Neurosurg. 1981; 54:323–330.
Article7. Ney JP, van der Goes DN. Evidence-based guideline update: Intraoperative spinal monitoring with somatosensory and transcranial electrical motor evoked potentials. Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology. 2012; 79:292.
Article8. Kothbauer KF, Deletis V, Epstein FJ. Motor-evoked potential monitoring for intramedullary spinal cord tumor surgery: correlation of clinical and neurophysiological data in a series of 100 consecutive procedures. Neurosurg Focus. 1998; 4:e1.
Article9. Sala F, Palandri G, Basso E, Lanteri P, Deletis V, Faccioli F, et al. Motor evoked potential monitoring improves outcome after surgery for intramedullary spinal cord tumors: a historical control study. Neurosurgery. 2006; 58:1129–1143.
Article10. Nuwer MR, Emerson RG, Galloway G, Legatt AD, Lopez J, Minahan R, et al. Evidence-based guideline update: intraoperative spinal monitoring with somatosensory and transcranial electrical motor evoked potentials: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology. 2012; 78:585–589.
Article11. Nash CL Jr, Lorig RA, Schatzinger LA, Brown RH. Spinal cord monitoring during operative treatment of the spine. Clin Orthop Relat Res. 1977; 100–105.
Article12. Calancie B, Madsen P, Lebwohl N. Stimulus-evoked EMG monitoring during transpedicular lumbosacral spine instrumentation Initial clinical results. Spine (Phila Pa 1976). 1994; 19:2780–2786.13. Danesh-Clough T, Taylor P, Hodgson B, Walton M. The use of evoked EMG in detecting misplaced thoracolumbar pedicle screws. Spine (Phila Pa 1976). 2001; 26:1313–1316.
Article14. Morota N, Deletis V, Constantini S, Kofler M, Cohen H, Epstein FJ. The role of motor evoked potentials during surgery for intramedullary spinal cord tumors. Neurosurgery. 1997; 41:1327–1336.
Article15. Sala F, Beltramello A, Gerosa M. Neuroprotective role of neurophysiological monitoring during endovascular procedures in the brain and spinal cord. Neurophysiol Clin. 2007; 37:415–421.
Article16. Deletis V. Intraoperative neurophysiology of the corticospinal tract of the spinal cord. Suppl Clin Neurophysiol. 2006; 59:107–112.17. Hyun SJ, Rhim SC. Combined motor and somatosensory evoked potential monitoring for intramedullary spinal cord tumor surgery: correlation of clinical and neurophysiological data in 17 consecutive procedures. Br J Neurosurg. 2009; 23:393–400.
Article18. Kearse LA Jr, Lopez-Bresnahan M, McPeck K, Tambe V. Loss of somatosensory evoked potentials during intramedullary spinal cord surgery predicts postoperative neurologic deficits in motor function [corrected]. J Clin Anesth. 1993; 5:392–398.
Article19. Ginsburg HH, Shetter AG, Raudzens PA. Postoperative paraplegia with preserved intraoperative somatosensory evoked potentials. Case report. J Neurosurg. 1985; 63:296–300.
Article20. Quiñones-Hinojosa A, Lyon R, Zada G, Lamborn KR, Gupta N, Parsa AT, et al. Changes in transcranial motor evoked potentials during intramedullary spinal cord tumor resection correlate with postoperative motor function. Neurosurgery. 2005; 56:982–993.21. Calancie B, Harris W, Brindle GF, Green BA, Landy HJ. Threshold-level repetitive transcranial electrical stimulation for intraoperative monitoring of central motor conduction. J Neurosurg. 2001; 95:2 Suppl. 161–168.
Article22. Skinner SA, Nagib M, Bergman TA, Maxwell RE, Msangi G. The initial use of free-running electromyography to detect early motor tract injury during resection of intramedullary spinal cord lesions. Neurosurgery. 2005; 56:2 Suppl. 299–314.
Article23. Hyun SJ, Rhim SC, Kang JK, Hong SH, Park BR. Combined motor-and somatosensory-evoked potential monitoring for spine and spinal cord surgery: correlation of clinical and neurophysiological data in 85 consecutive procedures. Spinal Cord. 2009; 47:616–622.
Article24. Jones SJ, Harrison R, Koh KF, Mendoza N, Crockard HA. Motor evoked potential monitoring during spinal surgery: responses of distal limb muscles to transcranial cortical stimulation with pulse trains. Electroencephalogr Clin Neurophysiol. 1996; 100:375–383.
Article25. Sutter M, Eggspuehler A, Grob D, Jeszenszky D, Benini A, Porchet F, et al. The validity of multimodal intraoperative monitoring (MIOM) in surgery of 109 spine and spinal cord tumors. Eur Spine J. 2007; 16:Suppl 2. S197–S208.
Article26. Albright AL. Intraoperative spinal cord monitoring for intramedullary surgery: an essential adjunct. Pediatr Neurosurg. 1998; 29:112.
Article27. Calancie B, Molano MR. Alarm criteria for motor-evoked potentials: what's wrong with the "presence-or-absence" approach? Spine (Phila Pa 1976). 2008; 33:406–414.28. Fehlings MG, Brodke DS, Norvell DC, Dettori JR. The evidence for intraoperative neurophysiological monitoring in spine surgery: does it make a difference? Spine (Phila Pa 1976). 2010; 35:9 Suppl. S37–S46.29. Hsu W, Bettegowda C, Jallo GI. Intramedullary spinal cord tumor surgery: can we do it without intraoperative neurophysiological monitoring? Childs Nerv Syst. 2010; 26:241–245.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Changes of motor evoked potentials and spinal cord evoked potentials following spinal cord injury in rats
- Intraoperative Neurophysiological Monitoring for Spinal Cord Tumor Surgery: Comparison of Motor and Somatosensory Evoked Potentials According to Tumor Types
- Intraoperative Monitoring for Tethered Cord Syndrome Using Somatosensory Evoked Potential and Motor Evoked Potential: Report of three cases
- The Clinical Significance of Somatosensory and Motor Evoked Potential in Myelopathy
- Monitoring of Motor and Somatosensory Evoked Potentials During Spine Surgery: Intraoperative Changes and Postoperative Outcomes
