Allergy Asthma Immunol Res.
2011 Apr;3(2):135-137. 10.4168/aair.2011.3.2.135.
Absence of Hyper-Responsiveness to Methacholine after Specific Bronchial Provocation Tests in a Worker With Hydroxyapatite-Induced Occupational Asthma
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Dong-A University, Busan, Korea. skleeai@dau.ac.kr
- 2Department of Occupational Medicine, College of Medicine, Dong-A University, Busan, Korea.
- KMID: 2130367
- DOI: http://doi.org/10.4168/aair.2011.3.2.135
Abstract
- Hydroxyapatite is commonly used as a filler to replace amputated bone or as a coating to promote bone ingrowth into prosthetic implants. Many modern implants, such as hip replacements and dental implants, are coated with hydroxyapatite. We report a patient with occupational asthma due to hydroxyapatite, proven by a specific inhalation challenge, who experienced an early asthmatic reaction after exposure to hydroxyapatite, without increased airway responsiveness to methacholine despite an increased eosinophil count in the peripheral blood. A 38-year-old male dental implant worker visited our allergy department for the evaluation of occupational asthma. He had treated dental implant titanium surfaces with hydroxyapatite for 1.5 years. One year after starting his employment, he noticed symptoms of rhinorrhea, paroxysmal cough, and chest tightness. His symptoms were aggravated during and shortly after work and subsided several hours after work. When he stopped working for 2 months because of his chest symptoms, he became asymptomatic. After restarting his work, his symptoms reappeared and were aggravated. A methacholine bronchial challenge test had a negative response. The following day, a specific bronchial provocation test with wheat powder was negative. On the third day, a specific bronchial provocation test with hydroxyapatite powder produced an early asthmatic response. On the fourth day, a methacholine bronchial challenge test was negative. Further studies are needed to evaluate the exact pathogenetic mechanism of hydroxyapatite-induced occupational asthma.
MeSH Terms
Figure
-
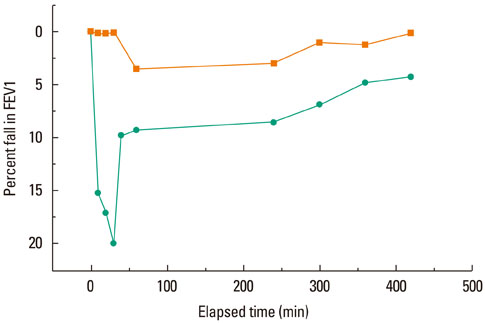
Fig. 1 Dose-response curves for the specific bronchial provocation tests with hydroxyapatite and placebo (rectangles, hydroxyapatite; circles, placebo). FEV1, forced expiratory volume in 1 second.
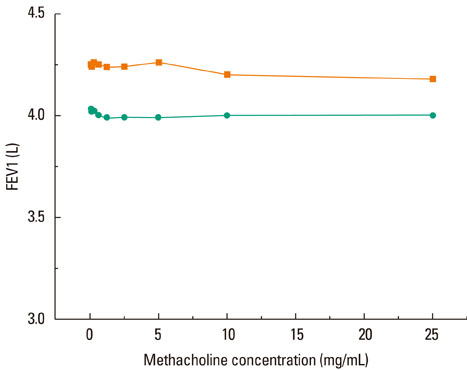
Fig. 2 Methacholine bronchial challenge tests on days 1 (top, orange rectangles) and 4 (bottom, green circles). On day 1, the baseline FEV1 was 4.31 L and the minimum FEV1 after methacholine inhalation was 4.18 L. On day 4, the baseline FEV1 was 4.0 L and the minimum FEV1 after methacholine inhalation was 3.99 L. FEV1, forced expiratory volume in 1 second.
Reference
-
1. Bernstein DI, Campo P, Baur X. Bernstein IL, Chan-Yeung M, Malo JL, Bernstein DI, editors. Clinical assessment and management of occupational asthma. Asthma in the workplace. 2006. 3rd ed. New York: Taylor & Francis;161–178.2. Malo JL, Chan-Yeung M. Occupational asthma. J Allergy Clin Immunol. 2001. 108:317–328.3. Lemiere C, Weytjens K, Cartier A, Malo JL. Late asthmatic reaction with airway inflammation but without airway hyperresponsiveness. Clin Exp Allergy. 2000. 30:415–417.4. Banks DE, Barkman HW Jr, Butcher BT, Hammad YY, Rando RJ, Glindmeyer HW 3rd, Jones RN, Weill H. Absence of hyperresponsiveness to methacholine in a worker with methylene diphenyl diisocyanate (MDI)-induced asthma. Chest. 1986. 89:389–393.5. Dykewicz MS. Occupational asthma: current concepts in pathogenesis, diagnosis, and management. J Allergy Clin Immunol. 2009. 123:519–528.6. Chai H, Farr RS, Froehlich LA, Mathison DA, McLean JA, Rosenthal RR, Sheffer AL, Spector SL, Townley RG. Standardization of bronchial inhalation challenge procedures. J Allergy Clin Immunol. 1975. 56:323–327.7. Cockcroft DW, Killian DN, Mellon JJ, Hargreave FE. Bronchial reactivity to inhaled histamine: a method and clinical survey. Clin Allergy. 1977. 7:235–243.8. Cockcroft DW, Davis BE, Todd DC, Smycniuk AJ. Methacholine challenge: comparison of two methods. Chest. 2005. 127:839–844.9. Todd DC, Davis BE, Hurst TS, Cockcroft DW. Dosimeter methacholine challenge: comparison of maximal versus submaximal inhalations. J Allergy Clin Immunol. 2004. 114:517–519.10. Allen ND, Davis BE, Hurst TS, Cockcroft DW. Difference between dosimeter and tidal breathing methacholine challenge: contributions of dose and deep inspiration bronchoprotection. Chest. 2005. 128:4018–4023.11. Gibson PG, Dolovich J, Denburg J, Ramsdale EH, Hargreave FE. Chronic cough: eosinophilic bronchitis without asthma. Lancet. 1989. 1:1346–1348.12. Hayes CW, Conway WF. Calcium hydroxyapatite deposition disease. Radiographics. 1990. 10:1031–1048.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Significant changes of bronchial responsiveness to methacholine after early asthmatic reaction to toluene diisocyanate (TDI) in a TDI-sensitive asthmatic worker
- The effect of nasal allergen challenge on the non- specific bronchial hyperresponsiveness
- Reactive dye induced occupational asthma without nonspecific bronchial hyperreactivity
- Association of Body Composition with the Development of Airway Hyper-Responsiveness
- Occupational asthma induced by tobacco leaf
