Allergy Asthma Immunol Res.
2011 Apr;3(2):118-122. 10.4168/aair.2011.3.2.118.
Challenge Test Results in Patients With Suspected Penicillin Allergy, but No Specific IgE
- Affiliations
-
- 1Allergy Unit, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark. h.mosbech@dadlnet.dk
- 2Allergy Clinic, Dermato-Allergological Department, Gentofte University Hospital, Hellerup, Denmark.
- KMID: 2130363
- DOI: http://doi.org/10.4168/aair.2011.3.2.118
Abstract
- PURPOSE
Patients with a history of allergic reaction to penicillin, but with no detectable specific IgE, are common and pose a dilemma. Challenge tests are considered to be the diagnostic gold standard. The aim of this study was to identify subgroups of patients with very low risk for reactions who could be safely tested using a more rapid and simple procedure.
METHODS
A total of 580 consecutively referred adult patients with a history of non-serious cutaneous allergic reactions to penicillin, but with no IgE, were challenged with therapeutic doses of penicillin V (phenoxymethylpenicillin), penicillin G (benzylpenicillin), or both.
RESULTS
Only 14 of 580 patients had a positive challenge test. In 11 of the 14, a reaction to challenge occurred within 2 hours, and none were anaphylactic. The year of the original reaction was known for 555 patients; a positive challenge was seen in only 0.4% of those with an original reaction >15 years before challenge, but in 4.6% of those with a more recent original reaction (P=0.001). Onset of a reaction within the first day of the original exposure was a predictive factor for a positive challenge (P=0.001) in patients challenged within 15 years of the original reaction.
CONCLUSIONS
Among suspected penicillin-allergic patients with non-severe skin reactions and no detectable specific IgE, the subgroup of patients who originally reacted more than 15 years previously had very low risk for reacting to a challenge. The risk was higher in patients with a more recent original reaction, especially if the symptoms had occurred within the first day of exposure.
MeSH Terms
Figure
-
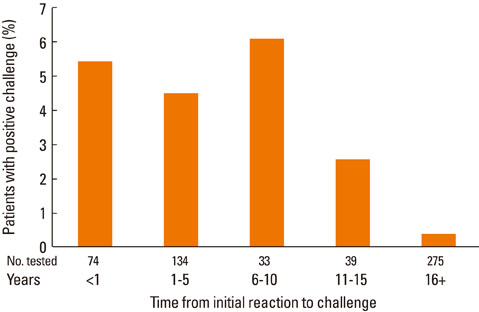
Fig. 1 Challenge outcomes according to the time interval between the original reaction and the challenge test.

Fig. 2 Challenge outcomes according to patient age at the time of the original reaction.
Reference
-
1. Demoly P, Bousquet J. Epidemiology of drug allergy. Curr Opin Allergy Clin Immunol. 2001. 1:305–310.2. Apter AJ, Kinman JL, Bilker WB, Herlim M, Margolis DJ, Lautenbach E, Hennessy S, Strom BL. Represcription of penicillin after allergic-like events. J Allergy Clin Immunol. 2004. 113:764–770.3. Lenler-Petersen P, Hansen D, Andersen M, Sørensen HT, Bille H. Drug-related fatal anaphylactic shock in Denmark 1968-1990. A study based on notifications to the Committee on Adverse Drug Reactions. J Clin Epidemiol. 1995. 48:1185–1188.4. Cars O, Mölstad S, Melander A. Variation in antibiotic use in the European Union. Lancet. 2001. 357:1851–1853.5. Ibia EO, Schwartz RH, Wiedermann BL. Antibiotic rashes in children: a survey in a private practice setting. Arch Dermatol. 2000. 136:849–854.6. Bigby M, Jick S, Jick H, Arndt K. Drug-induced cutaneous reactions. A report from the Boston Collaborative Drug Surveillance Program on 15,438 consecutive inpatients, 1975 to 1982. JAMA. 1986. 256:3358–3363.7. Apter AJ, Schelleman H, Walker A, Addya K, Rebbeck T. Clinical and genetic risk factors of self-reported penicillin allergy. J Allergy Clin Immunol. 2008. 122:152–158.8. Gomes ER, Demoly P. Epidemiology of hypersensitivity drug reactions. Curr Opin Allergy Clin Immunol. 2005. 5:309–316.9. Blanca-López N, Zapatero L, Alonso E, Torres MJ, Fuentes V, Martínez-Molero MI, Blanca M. Skin testing and drug provocation in the diagnosis of nonimmediate reactions to aminopenicillins in children. Allergy. 2009. 64:229–233.10. Goldberg A, Confino-Cohen R. Skin testing and oral penicillin challenge in patients with a history of remote penicillin allergy. Ann Allergy Asthma Immunol. 2008. 100:37–43.11. Messaad D, Sahla H, Benahmed S, Godard P, Bousquet J, Demoly P. Drug provocation tests in patients with a history suggesting an immediate drug hypersensitivity reaction. Ann Intern Med. 2004. 140:1001–1006.12. Bousquet PJ, Pipet A, Bousquet-Rouanet L, Demoly P. Oral challenges are needed in the diagnosis of β-lactam hypersensitivity. Clin Exp Allergy. 2008. 38:185–190.13. Torres MJ, Mayorga C, Leyva L, Guzman AE, Cornejo-García JA, Juarez C, Blanca M. Controlled administration of penicillin to patients with a positive history but negative skin and specific serum IgE tests. Clin Exp Allergy. 2002. 32:270–276.14. Antúnez C, Fernández T, Blanca-Lopez N, Torres MJ, Mayorga C, Canto G, Fernández J, Moya MC, Blanca M. IgE antibodies to betalactams: relationship between the triggering hapten and the specificity of the immune response. Allergy. 2006. 61:940–946.15. Fernández TD, Torres MJ, Blanca-López N, Rodríguez-Bada JL, Gomez E, Canto G, Mayorga C, Blanca M. Negativization rates of IgE radioimmunoassay and basophil activation test in immediate reactions to penicillins. Allergy. 2009. 64:242–248.16. Blanca M, Romano A, Torres MJ, Férnandez J, Mayorga C, Rodriguez J, Demoly P, Bousquet PJ, Merk HF, Sanz ML, Ott H, Atanasković-Marković M. Update on the evaluation of hypersensitivity reactions to betalactams. Allergy. 2009. 64:183–193.17. Vedsted P. Gender differences in the use of health care system. Ugeskr Laeger. 2007. 169:2403–2408.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis of food allergies: the impact of oral food challenge testing
- Evaluation of Banana Hypersensitivity Among a Group of Atopic Egyptian Children: Relation to Parental/Self Reports
- Utility of penicillin allergy testing in patients presenting with a history of penicillin allergy
- Food Allergy: Diagnosis and Management
- The Diagnosis of Food Allergy in a Pediatric Gastroenterology: Focusing on Non-IgE-mediated Allergic Diseases
