F-18 FDG PET-positive Fibrous Dysplasia in a Patient with Intestinal Non-Hodgkin's Lymphoma
- Affiliations
-
- 1Department of Internal Medicine, Hallym University Medical Center, Hallym University College of Medicine, Seoul, Korea. nep2n@hallym.or.kr
- 2Department of Orthopaedics, Hallym University Medical Center, Hallym University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Hallym University Medical Center, Hallym University College of Medicine, Seoul, Korea.
- 4Department of Nuclear Medicine, Hallym University Medical Center, Hallym University College of Medicine, Seoul, Korea.
- 5Department of Surgery, Hallym University Medical Center, Hallym University College of Medicine, Seoul, Korea.
Abstract
- Fibrous dysplasia (FD) is a common benign bone disorder of an unclear etiology. It is known that FD can appear without an increased FDG uptake on F-18 fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT). However, there are also several reports that FD showed increased FDG uptake and this mimicked malignant bone involvement on FDG-PET. Herein we describe a case of biopsy-proven FDG-PET positive FD in a patient with intestinal non-Hodgkin's lymphoma (NHL). A 45-year-old woman was diagnosed with intestinal NHL, which was removed by right hemicolectomy. After the operation, the FDG-PET/CT scan showed hypermetabolic activity in the right transverse process of the T10 vertebra. The patient then received a total of 6 cycles of R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone) chemotherapy every 3 weeks. After completion of the planned chemotherapy, the 2nd FDG-PET/CT showed increased FDG uptake (SUVmax=6.0 g/mL) of the previous bone lesion. The MR images revealed a T1-hypointense lesion with sharp borders in the same region, and this showed homogenous contrast enhancement on the fat-suppressed T1-weighted images. After the radiologic studies were carefully reviewed, the bone lesion was assumed to be benign such as FD. We performed bone biopsy and the histological examination confirmed the diagnosis of FD. In conclusion, bone lesions with FDG uptake need to be carefully interpreted when evaluating patients with known malignancy.
Keyword
MeSH Terms
Figure
-
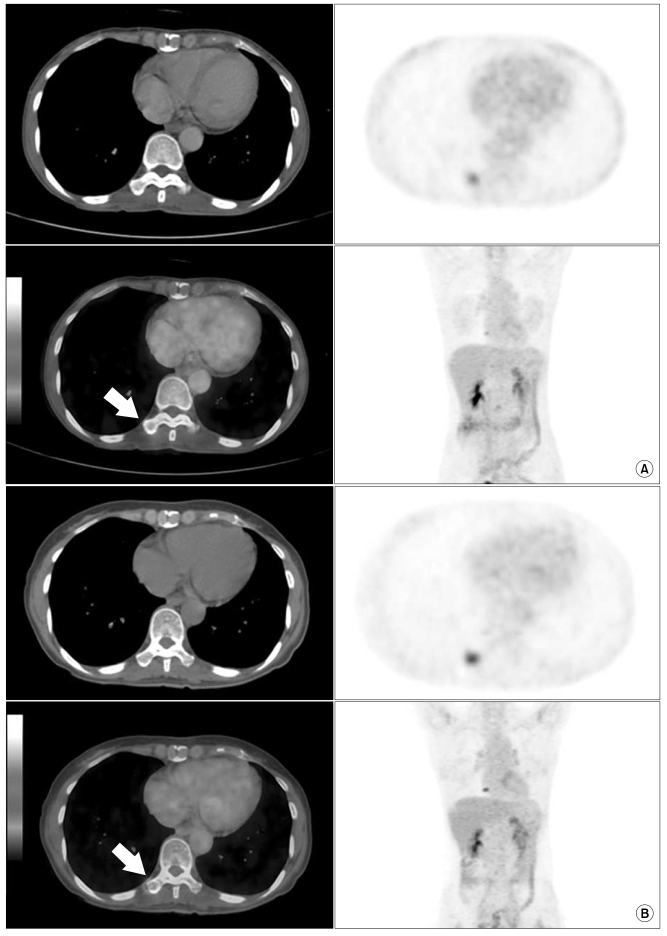
Fig. 1 (A) The initial FDG-PET/CT examination at the time of diagnosis of the diffuse large B-cell lymphoma demonstrates moderate FDG hypermetabolism (SUVmax=3.1 g/mL) in a right transverse process of the T10 vertebra (arrow). (B) Six months later after completion of the planned systemic chemotherapy, the follow-up PET/CT scan demonstrates further increased FDG hypermetabolic activity (SUVmax=6.0 g/mL) (arrow).
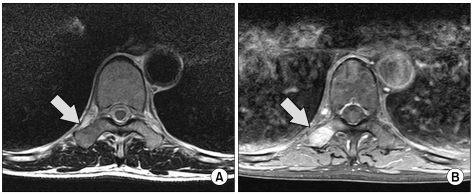
Fig. 2 The axial T1 weighted MR image shows a hypo-intense lesion (A, arrow) and the axial contrast-enhanced, fat-suppressed MR image shows homogeneous contrast enhancement of the well-defined lesion (B, arrow).
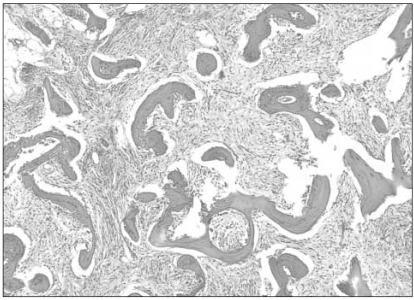
Fig. 3 Hematoxyline and eosin staining of the surgical biopsy specimen of the right transverse process of the T10 vertebra demonstrates bone trabeculae without osteoblastic rimming and there is bland spindle-cell proliferation. The bone trabeculae are composed of immature and disorganized osteoid (H & E, ×40).
Reference
-
1. Strobel K, Bode B, Lardinois D, Exner U. PET-positive fibrous dysplasia--a potentially misleading incidental finding in a patient with intimal sarcoma of the pulmonary artery. Skeletal Radiol. 2007; 36(Suppl 1):S24–S28. PMID: 16715239.2. Isohashi K, Tatsumi M, Higuchi I, Inoue A, Nakajo K, Ishikawa J, et al. 18F-FDG-PET in patients with malignant lymphoma having long-term follow-up: staging and restaging, and evaluation of treatment response and recurrence. Ann Nucl Med. 2008; 22:795–802. PMID: 19039558.
Article3. Strauss LG. Fluorine-18 deoxyglucose and false-positive results: a major problem in the diagnostics of oncological patients. Eur J Nucl Med. 1996; 23:1409–1415. PMID: 8781149.
Article4. Shigesawa T, Sugawara Y, Shinohara I, Fujii T, Mochizuki T, Morishige I. Bone metastasis detected by FDG PET in a patient with breast cancer and fibrous dysplasia. Clin Nucl Med. 2005; 30:571–573. PMID: 16024960.
Article5. Toba M, Hayashida K, Imakita S, Fukuchi K, Kume N, Shimotsu Y, et al. Increased bone mineral turnover without increased glucose utilization in sclerotic and hyperplastic change in fibrous dysplasia. Ann Nucl Med. 1998; 12:153–155. PMID: 9673717.
Article6. Stegger L, Juergens KU, Kliesch S, Wormanns D, Weckesser M. Unexpected finding of elevated glucose uptake in fibrous dysplasia mimicking malignancy: contradicting metabolism and morphology in combined PET/CT. Eur Radiol. 2007; 17:1784–1786. PMID: 17066288.
Article7. Charest M, Singnurkar A, Hickeson M, Novales JA, Derbekyan V. Intensity of FDG uptake is not everything: synchronous liposarcoma and fibrous dysplasia in the same patient on FDG PET-CT imaging. Clin Nucl Med. 2008; 33:455–458. PMID: 18580228.8. von Falck C, Rosenthal H, Laenger F, Lotz J, Knapp WH, Galanski M. Avid uptake of [(18)F]-FDG in fibrous dysplasia can mimic skeletal involvement in Hodgkin's disease. Eur J Nucl Med Mol Imaging. 2008; 35:223. PMID: 17874095.
Article9. Bonekamp D, Jacene H, Bartelt D, Aygun N. Conversion of FDG PET activity of fibrous dysplasia of the skull late in life mimicking metastatic disease. Clin Nucl Med. 2008; 33:909–911. PMID: 19033807.
Article10. Jee WH, Choi KH, Choe BY, Park JM, Shinn KS. Fibrous dysplasia: MR imaging characteristics with radiopathologic correlation. AJR Am J Roentgenol. 1996; 167:1523–1527. PMID: 8956590.
Article11. Zhibin Y, Quanyong L, Libo C, Jun Z, Hankui L, Jifang Z, et al. The role of radionuclide bone scintigraphy in fibrous dysplasia of bone. Clin Nucl Med. 2004; 29:177–180. PMID: 15162988.
Article12. Berrebi O, Steiner C, Keller A, Rougemont AL, Ratib O. F-18 fluorodeoxyglucose (FDG) PET in the diagnosis of malignant transformation of fibrous dysplasia in the pelvic bones. Clin Nucl Med. 2008; 33:469–471. PMID: 18580231.
Article13. Aoki J, Watanabe H, Shinozaki T, Takagishi K, Ishijima H, Oya N, et al. FDG PET of primary benign and malignant bone tumors: standardized uptake value in 52 lesions. Radiology. 2001; 219:774–777. PMID: 11376267.
Article14. Dimitrakopoulou-Strauss A, Strauss LG, Heichel T, Wu H, Burger C, Bernd L, et al. The role of quantitative (18)F-FDG PET studies for the differentiation of malignant and benign bone lesions. J Nucl Med. 2002; 43:510–518. PMID: 11937595.15. Eary JF, Mankoff DA. Tumor metabolic rates in sarcoma using FDG PET. J Nucl Med. 1998; 39:250–254. PMID: 9476930.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Versatile Role of 18 F-FDG PET/CT in a Patient with Pan-cerebellar Paraneoplastic Manifestation Due to Underlying Hodgkin’s Lymphoma
- Usefulness of F-18 FDG PET/CT in Staging of Peripheral T Cell Lymphoma
- Detection of Lymphomatous Marrow Infiltration using F-18 FDG PET at Initial Staging and after chemotherapy
- Extensive Extranodal Involvement of Rare Sites in Non Hodgkin's Lymphoma Detected on 18F- FDG PET-CT: A Case Report
- The Clinical Role of FDG PET in Malignant Lymphoma
