Modified Continuous Mucosal Connell Suture for the Pharyngeal Closure After Total Laryngectomy: Zipper Suture
- Affiliations
-
- 1Department of Otorhinolaryngology, Bursa Sevket Yilmaz Training and Research Hospital, Bursa, Turkey. drmehmethaksever@gmail.com
- KMID: 2117525
- DOI: http://doi.org/10.3342/ceo.2015.8.3.281
Abstract
OBJECTIVES
Pharyngocutaneous fistula is a serious complication after total laryngectomy, and there are some risk factors stated in the literature. The surgical suture techniques are not studied so much. The aim of this study is to evaluate the effectiveness of 'modified continuous mucosal Connell suture' on the incidence of pharyngocutaneous fistula after total laryngectomy.
METHODS
This is a retrospective case series study based at a tertiary center with 31 patients who underwent total laryngectomy between July 2011 and December 2013. Pharyngocutaneous fistula formation after total laryngectomy was evaluated with the patients who underwent modified continuous mucosal Connell suture for pharyngeal repair.
RESULTS
Pharyngocutaneous fistula was observed in only one patient (3.2%) who had a history of previous radiotherapy, and it was spontaneously healed within 6 days by conservative treatment.
CONCLUSION
We defined a new suture technique for the pharyngeal repair after total laryngectomy. This technique is a simple modification of continuous mucosal Connell suture. We named it as zipper suture. It is effective in the prevention of pharyngocutaneous fistula for pharyngeal reconstruction after total laryngectomy.
MeSH Terms
Figure
-
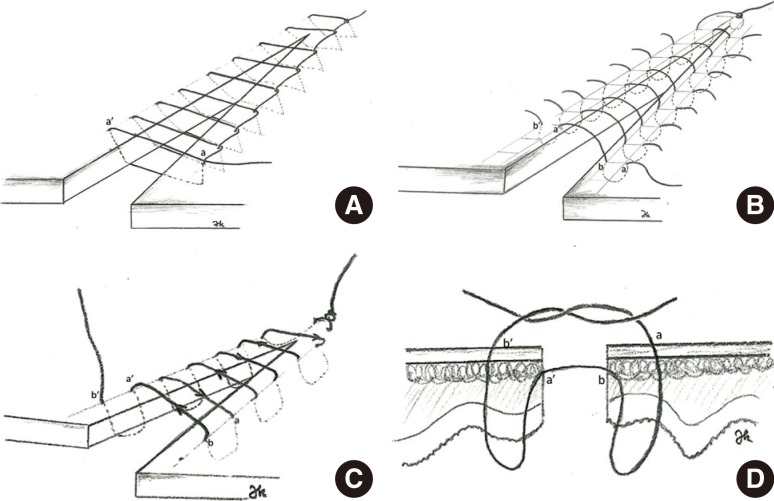
Fig. 1 Four different commonly used suture techniques; continuous interlocking (A), Lembert (B), Connell (C), and Gambia (D).
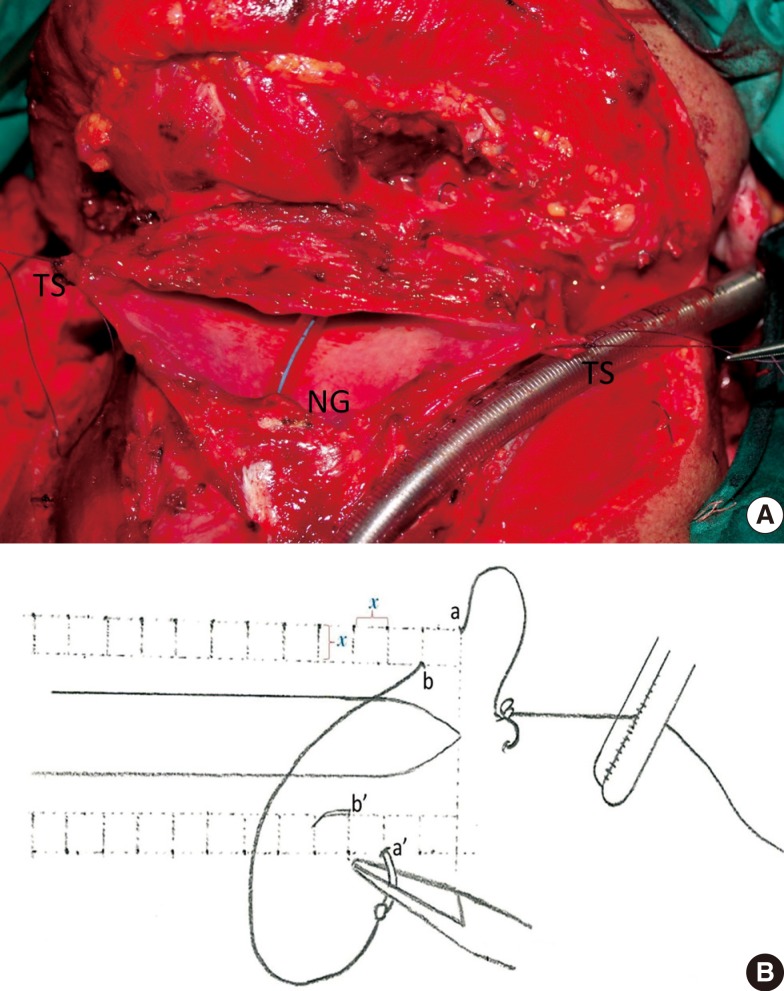
Fig. 2 (A) Pharyngeal defect after total laryngectomy. (B) Schematic diagram of the modified continuous Connell suture (zipper suture). Note that the distance (shown by χ in panel B) is preserved between every following stitch, and none of following stitches are on the same line vertically and horizontally. TS, tension suture; NG, nasogastric tube.
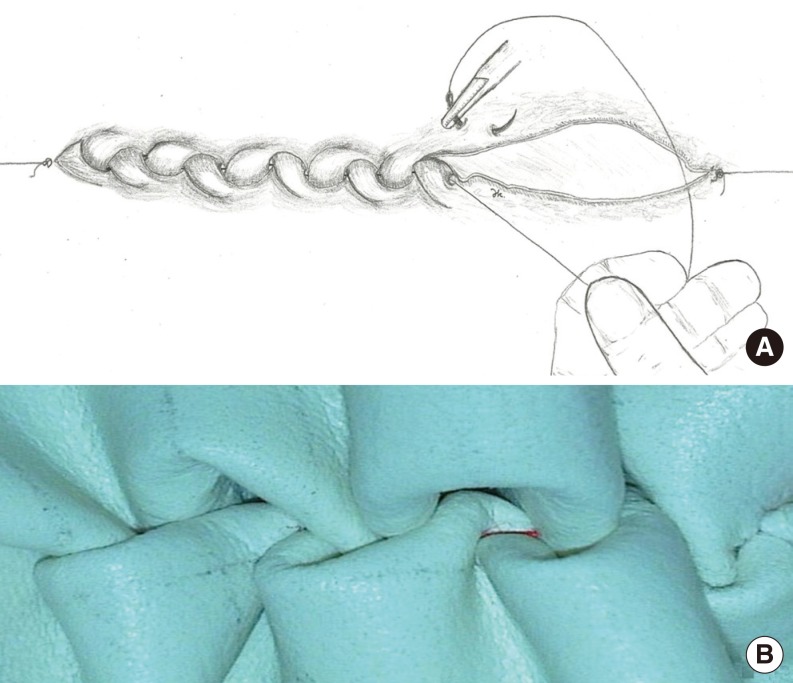
Fig. 3 Semi closed pharyngeal defect. Note that oblige position of porteque and needle. Assistant keeps the vicryl in tension to provide inversion of mucosa and not to permit relaxation. (A) Zipper suture on synthetic material. (B) Note that the spontaneous inversion of the edges.
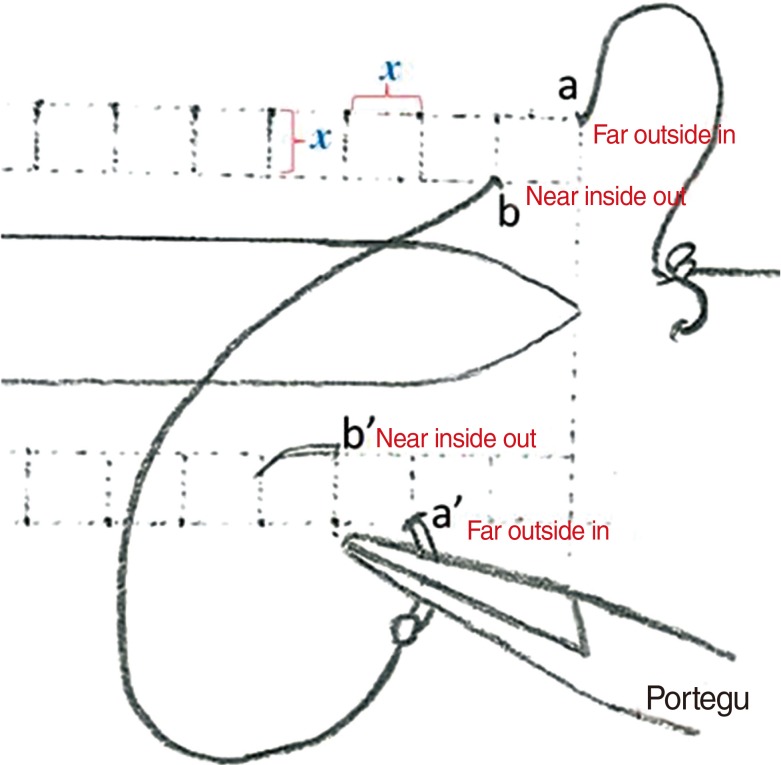
Fig. 4 Close-up view of the zipper suture technique. Note the stitch pattern of 'far outside in and near inside out'.
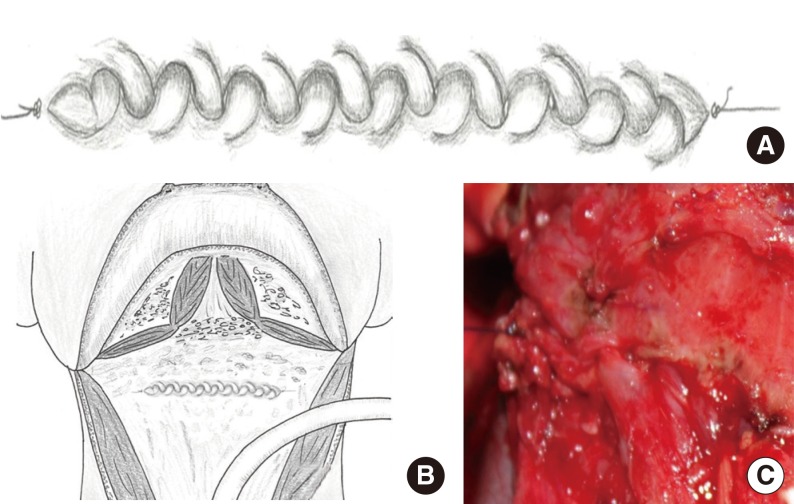
Fig. 5 Closed pharyngeal defect: schematic diagram of pharyngeal repair with zipper suture (A, B), pharyngeal repair of the case focused at suture line (C).
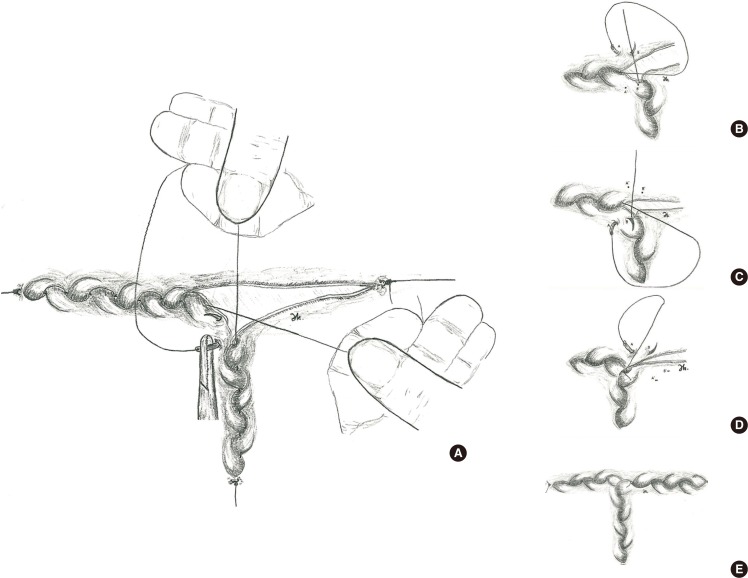
Fig. 6 (A-E) Schematic diagram of T type pharyngeal repair with zipper suture.
Cited by 1 articles
-
Externally Monitored Versus Conventional Buried Flaps in Laryngopharyngeal Reconstruction
Myung Jin Ban, Gina Na, Sungchul Ko, Joohyun Kim, Nam Hun Heo, Eun Chang Choi, Jae Hong Park, Won Shik Kim
Clin Exp Otorhinolaryngol. 2021;14(4):407-413. doi: 10.21053/ceo.2020.00234.
Reference
-
1. Saki N, Nikakhlagh S, Kazemi M. Pharyngocutaneous fistula after laryngectomy: incidence, predisposing factors, and outcome. Arch Iran Med. 2008; 5. 11(3):314–317. PMID: 18426323.2. Redaelli de Zinis LO, Ferrari L, Tomenzoli D, Premoli G, Parrinello G, Nicolai P. Postlaryngectomy pharyngocutaneous fistula: incidence, predisposing factors, and therapy. Head Neck. 1999; 3. 21(2):131–138. PMID: 10091981.
Article3. Altissimi G, Frenguelli A. Linear stapler closure of the pharynx during total laryngectomy: a 15-year experience (from closed technique to semi-closed technique). Acta Otorhinolaryngol Ital. 2007; 6. 27(3):118–122. PMID: 17883187.4. Bedrin L, Ginsburg G, Horowitz Z, Talmi YP. 25-year experience of using a linear stapler in laryngectomy. Head Neck. 2005; 12. 27(12):1073–1079. PMID: 16265656.
Article5. Goncalves AJ, de Souza JA Jr, Menezes MB, Kavabata NK, Suehara AB, Lehn CN. Pharyngocutaneous fistulae following total laryngectomy comparison between manual and mechanical sutures. Eur Arch Otorhinolaryngol. 2009; 11. 266(11):1793–1798. PMID: 19283399.
Article6. Lore JM, Medina J. An atlas of head and neck surgery. 4th ed. Philadelphia: Elsevier/Saunders;2004.7. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors. AJCC cancer staging manual. 7th ed. New York: Springer;2010.8. Akduman D, Naiboglu B, Uslu C, Oysu C, Tek A, Surmeli M, et al. Pharyngocutaneous fistula after total laryngectomy: incidence, predisposing factors, and treatment. Kulak Burun Bogaz Ihtis Derg. 2008; Nov-Dec. 18(6):349–354. PMID: 19293623.9. Virtaniemi JA, Kumpulainen EJ, Hirvikoski PP, Johansson RT, Kosma VM. The incidence and etiology of postlaryngectomy pharyngocutaneous fistulae. Head Neck. 2001; 1. 23(1):29–33.
Article10. Grau C, Johansen LV, Hansen HS, Andersen E, Godballe C, Andersen LJ, et al. Salvage laryngectomy and pharyngocutaneous fistulae after primary radiotherapy for head and neck cancer: a national survey from DAHANCA. Head Neck. 2003; 9. 25(9):711–716. PMID: 12953306.
Article11. Smith TJ, Burrage KJ, Ganguly P, Kirby S, Drover C. Prevention of postlaryngectomy pharyngocutaneous fistula: the Memorial University experience. J Otolaryngol. 2003; 8. 32(4):222–225. PMID: 14587560.
Article12. Rubino A, Gonzalez Aguilar O, Pardo HA, Simkim D, Vannelli A, Rossi A. Posttlaringectomy fistula: factors that favour its development. Rev Argent Cir. 2005; 88(5/6):234–241.13. Markou KD, Vlachtsis KC, Nikolaou AC, Petridis DG, Kouloulas AI, Daniilidis IC. Incidence and predisposing factors of pharyngocutaneous fistula formation after total laryngectomy. Is there a relationship with tumor recurrence? Eur Arch Otorhinolaryngol. 2004; 2. 261(2):61–67. PMID: 12856129.
Article14. Sarra LD, Rodriguez JC, Garcia Valea M, Bitar J, Da Silva A. Fistula following total laryngectomy. Retrospective study and bibliographical review. Acta Otorrinolaringol Esp. 2009; May-Jun. 60(3):186–189. PMID: 19558904.15. White HN, Golden B, Sweeny L, Carroll WR, Magnuson JS, Rosenthal EL. Assessment and incidence of salivary leak following laryngectomy. Laryngoscope. 2012; 8. 122(8):1796–1799. PMID: 22648757.
Article16. Sousa Ade A, Porcaro-Salles JM, Soares JM, de Moraes GM, Carvalho JR, Silva GS, et al. Predictors of salivary fistula after total laryngectomy. Rev Col Bras Cir. 2013; Mar-Apr. 40(2):98–103. PMID: 23752634.17. Aires FT, Dedivitis RA, Castro MA, Ribeiro DA, Cernea CR, Brandão LG. Pharyngocutaneous fistula following total laryngectomy. Braz J Otorhinolaryngol. 2012; 12. 78(6):94–98. PMID: 23306575.
Article18. Applebaum EL, Levine HL. Pharyngeal reconstruction after laryngectomy. Laryngoscope. 1977; 11. 87(11):1884–1890. PMID: 916783.
Article19. Lavelle RJ, Maw AR. The aetiology of post-laryngectomy pharyngo-cutaneous fistulae. J Laryngol Otol. 1972; 8. 86(8):785–793. PMID: 5044285.
Article20. Verma A, Panda NK, Mehta S, Mann SB, Mehra YN. Post laryngectomy complications and their mode of management: an analysis of 203 cases. Indian J Cancer. 1989; 12. 26(4):247–254. PMID: 2636211.21. Galli J, De Corso E, Volante M, Almadori G, Paludetti G. Postlaryngectomy pharyngocutaneous fistula: incidence, predisposing factors, and therapy. Otolaryngol Head Neck Surg. 2005; 11. 133(5):689–694. PMID: 16274794.
Article22. Calli C, Pinar E, Oncel S. Pharyngocutaneous fistula after total laryngectomy: less common with mechanical stapler closure. Ann Otol Rhinol Laryngol. 2011; 5. 120(5):339–344. PMID: 21675591.
Article23. Zhang X, Liu Z, Li Q, Liu X, Li H, Liu W, et al. Using a linear stapler for pharyngeal closure in total laryngectomy. Eur Arch Otorhinolaryngol. 2013; 3. 270(4):1467–1471. PMID: 22986414.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Astigmatism after Penetrating Keratoplasty According to Suture Methods
- An Experimental Study of Microvascular patency Using the Suture Techniques
- Secure and Convenient Three-point and Multi-point Suture Technique
- Pharyngeal Closure Reinforced With Sternohyoid and Omohyoid Muscle After Total Laryngectomy
- An experimental study on gross reactions of surrounding maxillary sutures to the widening of midpalatal suture in the dog
