Clinical Utility of an Automated Pupillometer in Patients with Acute Brain Lesion
- Affiliations
-
- 1Department of Neurosurgery, Konkuk University Medical Center, Seoul, Korea. ctmoon@kuh.ac.kr
- KMID: 2114374
- DOI: http://doi.org/10.3340/jkns.2015.58.4.363
Abstract
OBJECTIVE
The purpose of this study was to evaluate the clinical utility and validity of using a pupillometer to assess patients with acute brain lesions.
METHODS
Pupillary examinations using an automated pupillometer (NeurOptics(R)NPi(TM)-100 Pupillometer) were performed every 4 hours and were simultaneously assessed using the Glasgow Coma Scale (GCS) and for intracranial pressure (ICP), from admission to discharge or expire in neuro-intensive care unit (NICU). Manual pupillary examinations were also recorded for comparison. By comparing these data, we evaluated the validity of using automated pupillometers to predict clinical outcomes.
RESULTS
The mean values of the Neurologic Pupillary index (NPi) were different in the groups examined manually. The GCS correlated well with NPi values, especially in severe brain injury patients (GCS below 9). However, the NPi values were weakly correlated with intracranial pressure (ICP) when the ICP was lower than 30 cm H2O. The NPi value was not affected by age or intensity of illumination. In patients with a "poor" prognosis who had a Glasgow Outcome Scale (GOS) of 1 or 2, the mean initial NPi score was 0.88+/-1.68, whereas the value was 3.89+/-0.97 in patients with a "favorable" prognosis who had a GOS greater than 2 (p<0.001). For predicting clinical outcomes, the initial NPi value of 3.4 had the highest sensitivity and specificity.
CONCLUSION
An automated pupillometer can serve as a simple and useful tool for the accurate measurement of pupillary reactivity in patients with acute brain lesions.
MeSH Terms
Figure
-

Fig. 1 A : The shape of portable pupillometer. B : The display of pupillometer. MAX means the maximum pupil diameter before constriction. MIN means the pupil diameter at the peak of constriction. %CH means the percent of the change (MAX-MIN)/MAX. LAT means the latency and it represents the time of the onset of the constriction. CV, MCV means the average and the maximum constriction velocity. DV means the dilation velocity. The graph below the table depicts change of size of pupil according to change of time.
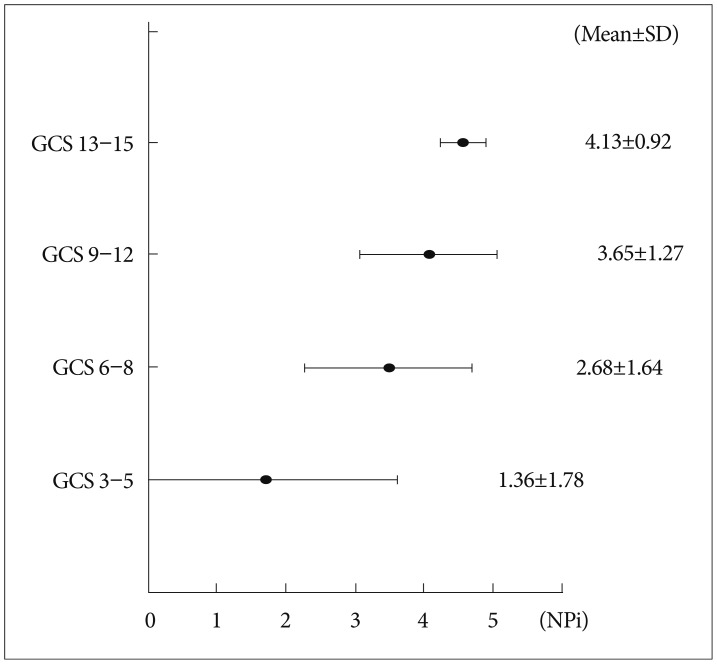
Fig. 2 The graph presents the mean value of the Neurologic Pupillary index (NPi) in four groups divided according to the Glasgow Coma Scale (GCS). The NPi value tends to decrease as the GCS decreases, especially in the "poor" clinical group with a GCS of 3 to 5.

Fig. 3 There is no relationship between NPi and ICP when ICP is lower than 30 cm H2O. However, the NPi value significantly decreased when ICP was higher than 30 cm H2O. NPi : Neurologic Pupillary index, ICP : intracranial pressure.

Fig. 4 The closer the curve to the left upper angular point, the more reliable the test becomes. This ROC curve shows the AUC of 0.92, and both sensitivity and specificity are optimal when the NPi cut-off value is 3.4 (starred dot). ROC : receiver operating characteristic, AUC : area under the curve, NPi : Neurologic Pupillary index.
Cited by 1 articles
-
Quantitative assessments of pupillary light reflexes in neurocritically ill patients
Tae Jung Kim
J Neurocrit Care. 2022;15(2):79-87. doi: 10.18700/jnc.220085.
Reference
-
1. Behrends M, Niemann CU, Larson MD. Infrared pupillometry to detect the light reflex during cardiopulmonary resuscitation : a case series. Resuscitation. 2012; 83:1223–1228. PMID: 22659054.
Article2. Chang DS, Arora KS, Boland MV, Supakontanasan W, Friedman DS. Development and validation of an associative model for the detection of glaucoma using pupillography. Am J Ophthalmol. 2013; 156:1285–1296.e2. PMID: 24011523.
Article3. Chen JW, Gombart ZJ, Rogers S, Gardiner SK, Cecil S, Bullock RM. Pupillary reactivity as an early indicator of increased intracranial pressure : the introduction of the Neurological Pupil index. Surg Neurol Int. 2011; 2:82. PMID: 21748035.
Article4. Chen JW, Vakil-Gilani K, Williamson KL, Cecil S. Infrared pupillometry, the Neurological Pupil index and unilateral pupillary dilation after traumatic brain injury : implications for treatment paradigms. Springerplus. 2014; 3:548. PMID: 25332854.5. Cohen LM, Rosenberg MA, Tanna AP, Volpe NJ. A novel computerized portable pupillometer detects and quantifies relative afferent pupillary defects. Curr Eye Res. 2015; 40:1120–1127. PMID: 25658805.
Article6. Connelly MA, Brown JT, Kearns GL, Anderson RA, St Peter SD, Neville KA. Pupillometry : a non-invasive technique for pain assessment in paediatric patients. Arch Dis Child. 2014; 99:1125–1131. PMID: 25187497.
Article7. Fletcher GC, Asbury AJ, Brown JH. Pupil changes during cardiopulmonary bypass. Br J Anaesth. 1996; 76:20–22. PMID: 8672373.
Article8. Hults KN, Knowlton SL, Oliver JW, Wolfson T, Gamst A. A study of pupillary assessment in outpatient neurosurgical clinics. J Neurosci Nurs. 2006; 38:447–452. PMID: 17233516.
Article9. Kim J, Heo J, Ji D, Kim MS. Quantitative assessment of pupillary light reflex in normal and anesthetized dogs : a preliminary study. J Vet Med Sci. 2015; 77:475–478. PMID: 25648149.
Article10. Kramer CL, Rabinstein AA, Wijdicks EF, Hocker SE. Neurologist versus machine : is the pupillometer better than the naked eye in detecting pupillary reactivity. Neurocrit Care. 2014; 21:309–311. PMID: 24865269.
Article11. Larson MD, Muhiudeen I. Pupillometric analysis of the 'absent light reflex'. Arch Neurol. 1995; 52:369–372. PMID: 7710372.
Article12. Marmarou A, Lu J, Butcher I, McHugh GS, Murray GD, Steyerberg EW, et al. Prognostic value of the Glasgow Coma Scale and pupil reactivity in traumatic brain injury assessed pre-hospital and on enrollment : an IMPACT analysis. J Neurotrauma. 2007; 24:270–280. PMID: 17375991.
Article13. Meeker M, Du R, Bacchetti P, Privitera CM, Larson MD, Holland MC, et al. Pupil examination : validity and clinical utility of an automated pupillometer. J Neurosci Nurs. 2005; 37:34–40. PMID: 15794443.14. Narayan RK, Greenberg RP, Miller JD, Enas GG, Choi SC, Kishore PR, et al. Improved confidence of outcome prediction in severe head injury. A comparative analysis of the clinical examination, multimodality evoked potentials, CT scanning, and intracranial pressure. J Neurosurg. 1981; 54:751–762. PMID: 7241184.15. Shindler KS, Revere K, Dutt M, Ying GS, Chung DC. In vivo detection of experimental optic neuritis by pupillometry. Exp Eye Res. 2012; 100:1–6. PMID: 22561341.16. Taylor WR, Chen JW, Meltzer H, Gennarelli TA, Kelbch C, Knowlton S, et al. Quantitative pupillometry, a new technology : normative data and preliminary observations in patients with acute head injury. Technical note. J Neurosurg. 2003; 98:205–213. PMID: 12546375.
Article17. Theodossiadis PG, Achtsidis V, Theodoropoulou S, Tentolouris N, Komninos C, Fountas KN. The effect of alpha antagonists on pupil dynamics : implications for the diagnosis of intraoperative floppy iris syndrome. Am J Ophthalmol. 2012; 153:620–626. PMID: 22265152.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Automatic Pupillometer and Pupil Card for Measuring Pupil Size
- Quantitative Pupillometry of the Pupillary Light Reflex in Koreans
- Correlates of Depression and Anxiety in Acute Stroke Patients
- Preoperative Evaluation of Brain Lesion with 201Tl Brain SPECT: Is It Useful to Differentiate Benign and Malignant Lesions?
- Comparison of Colvardpupillometer, ORBScan II and Sirius in Determining Pupil Size for Refractive Surgery
