Comparative Study between Axial and Coronal Planes of CT Enterography in Evaluation of Disease Activity and Complications of Crohn Disease
- Affiliations
-
- 1Department of Diagnostic Radiology, Kyung Hee University Hospital, Seoul, Korea. indawn@hanafos.com
- 2Department of Gastroenterology, Kyung Hee University Hospital, Seoul, Korea.
- KMID: 2097988
- DOI: http://doi.org/10.3348/jksr.2013.68.2.107
Abstract
- PURPOSE
To retrospectively compare the accuracy of axial and coronal planes of CT enterography for detection of pathologic findings of Crohn disease.
MATERIALS AND METHODS
168 patients who were suspected of having Crohn disease underwent CT enterography. 66 patients who were diagnosed Crohn disease were retrospectively evaluated (endoscopic biopsy of terminal ileum: 12 patients, segmental resection of small bowel: 6 patients, diagnosed based on a combination of clinical, histopathological and imaging findings: 48 patients). 2 radiologists reviewed axial planes of CT enterography and one month later reviewed coronal planes. CT enterography findings of active phase, chronic phase and complications of Crohn disease were evaluated and then compared with axial and coronal planes by using chi-square test.
RESULTS
Mucosal hyperenhancement, wall thickening, and mesenteric fat stranding were more detected on axial planes, which were CT findings of active Crohn disease. Pseudosacculation, fibrotic strictures, fistulas, abscesses were more detected on coronal planes, which were CT findings of chronic Crohn disease or complications. In particular, pseudosacculation and fibrotic strictures were significantly more detected on coronal planes.
CONCLUSION
When evaluating CT enterography in Crohn disease, coronal planes provide more useful diagnostic information of pseudosacculation and fibrotic strictures.
Figure
-
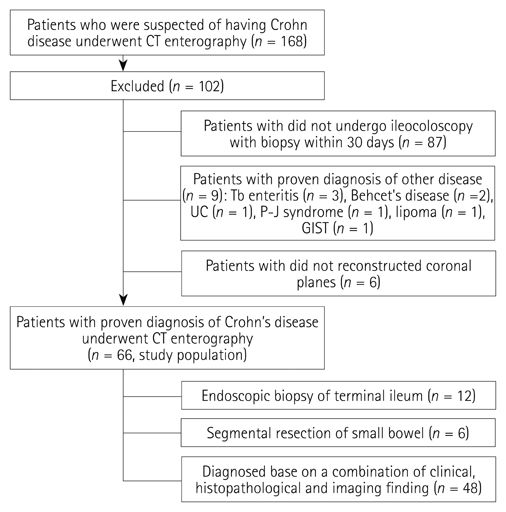
Fig. 1 Flowchart of the selection of patients for retrospective study, with all patients undergoing CT enterography and ileocoloscopy with biopsy within 30 days. Note.-GIST = gastrointestinal stromal tumor, P-J syndrome = Peutz-Jegher syndrome, Tb enteritis = Tuberculous enteritis, UC = ulcerative colitis

Fig. 2 A 19-year-old man with Crohn disease at the ileum. CT enterogram shows concentric wall thickening and mucosal hyperenhancement (arrows) at the ileum on axial image (A), which were missed on coronal image (B).

Fig. 3 A 24-year-old man with active Crohn disease at the ascending colon and ileum. A, B. CT enterogram shows concentric wall thickening and mucosal hyperenhancement (arrows) at the ileum on axial image. The thickened wall has a stratified appearance. CT enterography also shows increased attenuation of the mesenteric fat on axial image, which was not shown on coronal image. C. Endoscopy image shows erythematous mucosal change at the ileocecal valve. D. Image from barium study demonstrates transient luminal narrowing, mucosal fold widening and thickening on the proximal ascending colon and the terminal ileum.

Fig. 4 A 31-year-old man with long-standing Crohn disease at the ileum. CT enterogram shows typical straightening of the mesenteric boder (arrows), a finding that indicates linear ulceration or ulcer scar and pseudosacculation of the antimesenteric border (arrowhead) at the ileum on coronal image.
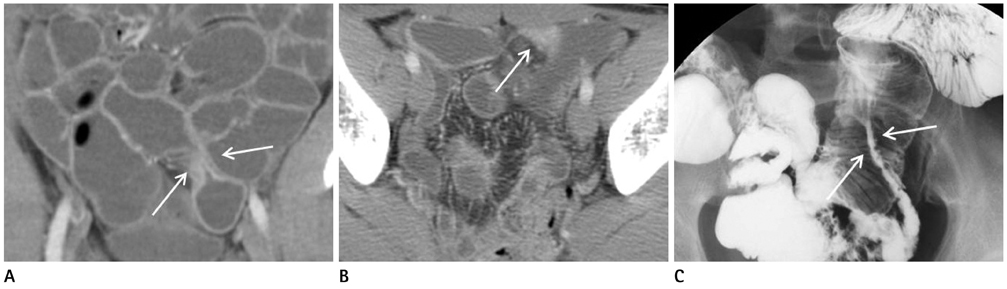
Fig. 5 A 27-year-old man with fibrotic stricture in Crohn disease. A, B. CT enterogram shows fibrotic stricture (arrows) at the pelvic ileal loop on coronal image, which was missed on axial image. C. Image from barium study also shows typical fibrotic stricture (arrows) at the pelvic ileal loop.
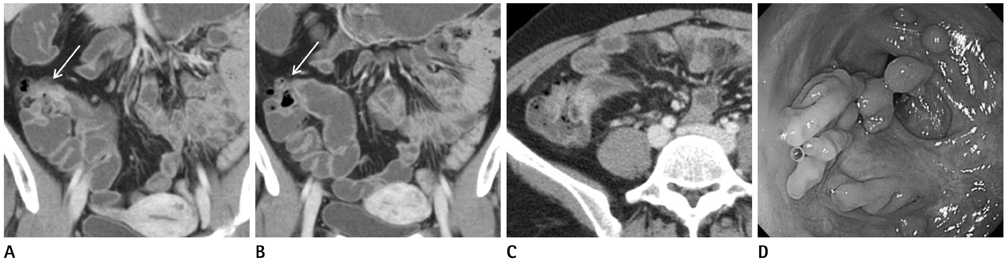
Fig. 6 A 27-year-old woman with fibrotic stricture in Crohn disease. A-C. CT enterogram shows fibrotic stricture (arrows) at the ileocecal (IC) valve with dilatation of terminal ileum on serial coronal images, which was missed on axial image. D. Endoscopy image shows numerous pseudopolyp and cecal deformity. Scope couldn't be passed of stenotic portion of IC valve.
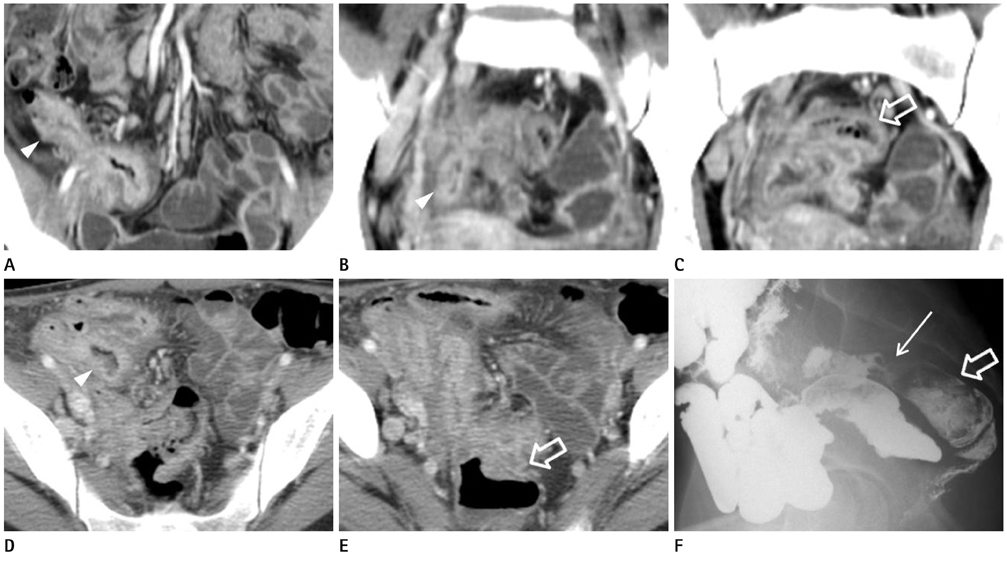
Fig. 7 A 23-year-old woman with ileo-colonic fistula in Crohn disease. A-E. CT enterography shows ileo-colonic fistula on serial coronal images, which was missed on axial image. Fistula extends from the distal ileum (arrowheads) to the adjacent distal sigmoid colon (open arrows). F. Image from barium study obtained after 4 hours, demonstrates ileocolonic fistula on sagittal image (arrow). Sigmoid colon (open arrow) and rectum are seen.
Reference
-
1. Furukawa A, Saotome T, Yamasaki M, Maeda K, Nitta N, Takahashi M, et al. Cross-sectional imaging in Crohn disease. Radiographics. 2004. 24:689–702.2. Jaffe TA, Martin LC, Thomas J, Adamson AR, DeLong DM, Paulson EK. Small-bowel obstruction: coronal reformations from isotropic voxels at 16-section multi-detector row CT. Radiology. 2006. 238:135–142.3. Jaffe TA, Martin LC, Miller CM, Franklin KM, Merkle EM, Thompson WM, et al. Abdominal pain: coronal reformations from isotropic voxels with 16-section CT--reader lesion detection and interpretation time. Radiology. 2007. 242:175–181.4. Wold PB, Fletcher JG, Johnson CD, Sandborn WJ. Assessment of small bowel Crohn disease: noninvasive peroral CT enterography compared with other imaging methods and endoscopy--feasibility study. Radiology. 2003. 229:275–281.5. Elsayes KM, Al-Hawary MM, Jagdish J, Ganesh HS, Platt JF. CT enterography: principles, trends, and interpretation of findings. Radiographics. 2010. 30:1955–1970.6. Booya F, Fletcher JG, Huprich JE, Barlow JM, Johnson CD, Fidler JL, et al. Active Crohn disease: CT findings and interobserver agreement for enteric phase CT enterography. Radiology. 2006. 241:787–795.7. Goldberg HI, Gore RM, Margulis AR, Moss AA, Baker EL. Computed tomography in the evaluation of Crohn disease. AJR Am J Roentgenol. 1983. 140:277–282.8. Lee SS, Ha HK, Yang SK, Kim AY, Kim TK, Kim PN, et al. CT of prominent pericolic or perienteric vasculature in patients with Crohn's disease: correlation with clinical disease activity and findings on barium studies. AJR Am J Roentgenol. 2002. 179:1029–1036.9. Horton KM, Fishman EK. The current status of multidetector row CT and three-dimensional imaging of the small bowel. Radiol Clin North Am. 2003. 41:199–212.10. Paulsen SR, Huprich JE, Fletcher JG, Booya F, Young BM, Fidler JL, et al. CT enterography as a diagnostic tool in evaluating small bowel disorders: review of clinical experience with over 700 cases. Radiographics. 2006. 26:641–657. discussion 657-662.11. Maglinte DD, Sandrasegaran K, Lappas JC, Chiorean M. CT Enteroclysis. Radiology. 2007. 245:661–671.12. Hara AK, Leighton JA, Heigh RI, Sharma VK, Silva AC, De Petris G, et al. Crohn disease of the small bowel: preliminary comparison among CT enterography, capsule endoscopy, small-bowel follow-through, and ileoscopy. Radiology. 2006. 238:128–134.13. Tolan DJ, Greenhalgh R, Zealley IA, Halligan S, Taylor SA. MR enterographic manifestations of small bowel Crohn disease. Radiographics. 2010. 30:367–384.14. Schmidt S, Lepori D, Meuwly JY, Duvoisin B, Meuli R, Michetti P, et al. Prospective comparison of MR enteroclysis with multidetector spiral-CT enteroclysis: interobserver agreement and sensitivity by means of "sign-by-sign" correlation. Eur Radiol. 2003. 13:1303–1311.15. Bodily KD, Fletcher JG, Solem CA, Johnson CD, Fidler JL, Barlow JM, et al. Crohn Disease: mural attenuation and thickness at contrast-enhanced CT Enterography--correlation with endoscopic and histologic findings of inflammation. Radiology. 2006. 238:505–516.16. Hara AK, Alam S, Heigh RI, Gurudu SR, Hentz JG, Leighton JA. Using CT enterography to monitor Crohn's disease activity: a preliminary study. AJR Am J Roentgenol. 2008. 190:1512–1516.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of Computed Tomography Enterography/Magnetic Resonance Enterography: Is It in Prime Time?
- Pediatric Magnetic Resonance Enterography: Focused on Crohn's Disease
- Need of Two Planes of CT Scan for Evaluation of Orbital Blowout Fracture Reconstruction
- Computed Tomography Enterography and Magnetic Resonance Enterography in the Diagnosis of Crohn's Disease
- Preparation, Technique, and Imaging of Computed Tomography/Magnetic Resonance Enterography
