A Dual Expandable Stent for Treatment of Malignant Colorectal Obstruction: Long-Term Follow-Up Results
- Affiliations
-
- 1Department of Radiology, Kosin University College of Medicine, Gospel Hospital, Busan, Korea. gsjung@medimail.co.kr
- KMID: 2097978
- DOI: http://doi.org/10.3348/jksr.2012.67.6.433
Abstract
- PURPOSE
To analyze the long-term results and to evaluate the efficacy of a dual expandable stent for the treatment of malignant colorectal strictures.
MATERIALS AND METHODS
Under the fluoroscopic guidance, stents were placed in 60 patients with malignant colorectal strictures. A dual stent consists of two stents, the outer stent was placed into the stricture which was followed by coaxial placement of the inner bare stent. Technical and clinical success rates, complications, patient survival and stent patency during the follow-up period were evaluated in this study.
RESULTS
Stent placement was technically successful in 57 of 60 patients (95%). Of them, obstructive symptoms resolved within two days in 12/12 (100%) patients in the preoperative group and in 36/45 (80%) patients in the palliative group. Complications associated with this procedure were perforation (n = 5), migration (n = 3), and tumor overgrowth (n = 2). Each of the six patients in the preoperative group underwent conventional laparotomy and laparoscopic surgery, respectively. The mean interval between stent insertion and surgery was nine days. In the palliative group, the median survival was 159 days (mean; 235) and the median patency of stent was 116 days (mean; 185). 1-month, 3-month, 6-month, 12-month and 24-month stent patency were 75%, 60%, 27%, 13% and 7%, respectively.
CONCLUSION
Insertion of a dual expandable nitinol stent into malignant colorectal obstruction is a safe and effective procedure for the palliative treatment of malignant colorectal obstruction. This procedure is also effective for preoperative decompression.
MeSH Terms
Figure
-
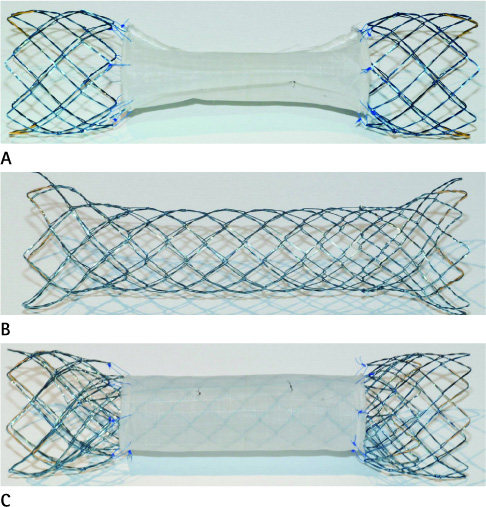
Fig. 1 Photographs of dual expandable nitinol stent. A. An outer partially covered stent. B. An inner bare nitinol stent. C. An assembled dual expandable nitinol stent.
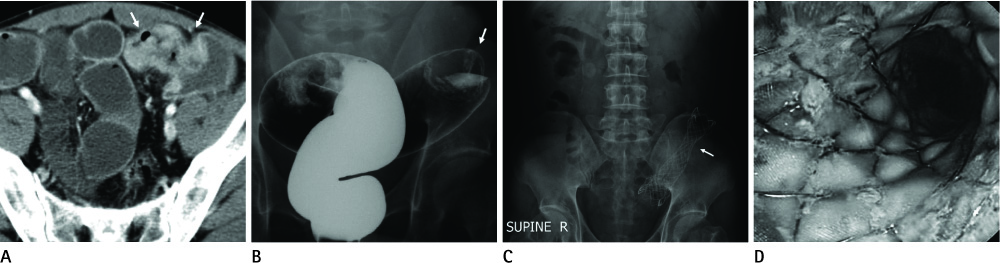
Fig. 2 Sigmoid colon cancer in a 43-year-old man. A. Contrast enhanced axial CT image shows a focal mucosal thickening and apple-core like luminal narrowing in the sigmoid colon (arrows). B. Double contrast barium study shows a total obstruction at the sigmoid colon (arrow). C. Abdominal plain radiograph obtained two days after the procedure shows full expansion of the stent (arrow) and normal pattern of bowel gas. D. Follow-up sigmoidoscopy shows the patent stented lumen.
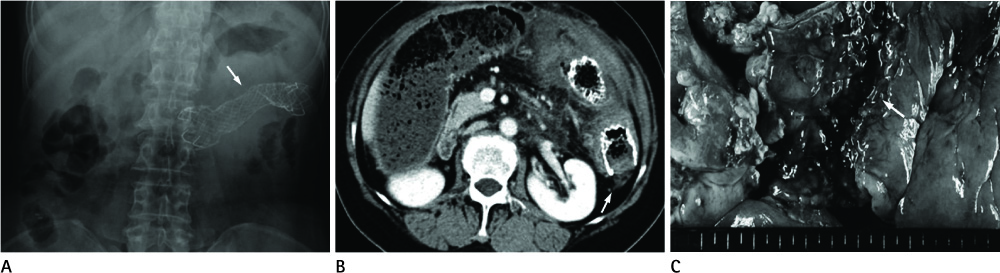
Fig. 3 Ovarian cancer with colon metastasis in a 68-year-old woman. A. A plain radiograph obtained two days after the procedure shows the expanded stent in left upper quadrant of the abdomen (arrow). B. Contrast enhanced CT scan obtained five days after the procedure shows that distal portion of the stent abuts against the bowel wall, causing perforation (arrow). C. Photograph of the specimen obtained at emergency surgery 5 days after stent insertion shows the perforation site (arrow).

Fig. 4 Kaplan-Meier estimation of patient survival rate.
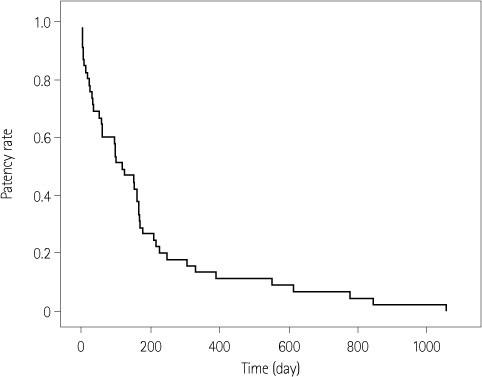
Fig. 5 Kaplan-Meier estimation of stent patency rate.
Reference
-
1. Deans GT, Krukowski ZH, Irwin ST. Malignant obstruction of the left colon. Br J Surg. 1994. 81:1270–1276.2. Baron TH. Expandable metal stents for the treatment of cancerous obstruction of the gastrointestinal tract. N Engl J Med. 2001. 344:1681–1687.3. Jung GS, Song HY, Kang SG, Huh JD, Park SJ, Koo JY, et al. Malignant gastroduodenal obstructions: treatment by means of a covered expandable metallic stent-initial experience. Radiology. 2000. 216:758–763.4. Song HY, Kim JH, Shin JH, Kim HC, Yu CS, Kim JC, et al. A dual-design expandable colorectal stent for malignant colorectal obstruction: results of a multicenter study. Endoscopy. 2007. 39:448–454.5. Mauro MA, Koehler RE, Baron TH. Advances in gastrointestinal intervention: the treatment of gastroduodenal and colorectal obstructions with metallic stents. Radiology. 2000. 215:659–669.6. Camúñez F, Echenagusia A, Simó G, Turégano F, Vázquez J, Barreiro-Meiro I. Malignant colorectal obstruction treated by means of self-expanding metallic stents: effectiveness before surgery and in palliation. Radiology. 2000. 216:492–497.7. Athreya S, Moss J, Urquhart G, Edwards R, Downie A, Poon FW. Colorectal stenting for colonic obstruction: the indications, complications, effectiveness and outcome--5 year review. Eur J Radiol. 2006. 60:91–94.8. Kim JH, Song HY, Li YD, Shin JH, Park JH, Yu CS, et al. Dual-design expandable colorectal stent for malignant colorectal obstruction: comparison of flared ends and bent ends. AJR Am J Roentgenol. 2009. 193:248–254.9. Franklin ME Jr, Rosenthal D, Abrego-Medina D, Dorman JP, Glass JL, Norem R, et al. Prospective comparison of open vs. laparoscopic colon surgery for carcinoma. Five-year results. Dis Colon Rectum. 1996. 39:10 Suppl. S35–S46.10. Kang SG, Jung GS, Cho SG, Kim JG, Oh JH, Song HY, et al. The efficacy of metallic stent placement in the treatment of colorectal obstruction. Korean J Radiol. 2002. 3:79–86.11. Lee JH, Ross WA, Davila R, Chang G, Lin E, Dekovich A, et al. Self-expandable metal stents (SEMS) can serve as a bridge to surgery or as a definitive therapy in patients with an advanced stage of cancer: clinical experience of a tertiary cancer center. Dig Dis Sci. 2010. 55:3530–3536.12. Martinez-Santos C, Lobato RF, Fradejas JM, Pinto I, Ortega-Deballón P, Moreno-Azcoita M. Self-expandable stent before elective surgery vs. emergency surgery for the treatment of malignant colorectal obstructions: comparison of primary anastomosis and morbidity rates. Dis Colon Rectum. 2002. 45:401–406.13. Baron TH, Dean PA, Yates MR 3rd, Canon C, Koehler RE. Expandable metal stents for the treatment of colonic obstruction: techniques and outcomes. Gastrointest Endosc. 1998. 47:277–286.14. Park JK, Lee MS, Ko BM, Kim HK, Kim YJ, Choi HJ, et al. Outcome of palliative self-expanding metal stent placement in malignant colorectal obstruction according to stent type and manufacturer. Surg Endosc. 2011. 25:1293–1299.15. Kim JH, Song HY, Shin JH, Choi E, Kim TW, Lee SK, et al. Stent collapse as a delayed complication of placement of a covered gastroduodenal stent. AJR Am J Roentgenol. 2007. 188:1495–1499.16. Sebastian S, Johnston S, Geoghegan T, Torreggiani W, Buckley M. Pooled analysis of the efficacy and safety of self-expanding metal stenting in malignant colorectal obstruction. Am J Gastroenterol. 2004. 99:2051–2057.17. Morino M, Bertello A, Garbarini A, Rozzio G, Repici A. Malignant colonic obstruction managed by endoscopic stent decompression followed by laparoscopic resections. Surg Endosc. 2002. 16:1483–1487.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Dual Expandable Nitinol Stent: The Long-term Results in Patients with Malignant Gastroduodenal Strictures
- Endoscopic Management of Malignant Colonic Obstruction
- Dual-Design Expandable Colorectal Stent for a Malignant Colorectal Obstruction: Preliminary Prospective Study Using New 20-mm Diameter Stents
- Fluoroscopic Stent Placement as a Bridge to Surgery for Malignant Colorectal Obstruction: Short- and Long-Term Outcomes
- Usefulness of a Self-expandable Nitinol Stent Through an Endoscope for the Treatment of a Malignant Colorectal Obstruction
