Review of Breast Cancers That Can Mimic a Cystic Component: Ultrasonographic and Pathologic Correlations
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Hospital, Korea. ywchang@hosp.sch.ac.kr
- 2Department of Radiology, Soonchunhyang Cheonan Hospital, Korea.
- 3Department of Radiology, Soonchunhyang Gumi Hospital, Korea.
- 4Department of Pathology, Soonchunhyang University Hospital, Korea.
- KMID: 2097950
- DOI: http://doi.org/10.3348/jksr.2011.64.3.273
Abstract
- We illustrate the sonographic findings of malignant breast masses that can mimic a cystic component with pathologic correlations. The disease entities presented in this study include infiltrating ductal carcinoma, ductal carcinoma in situ (DCIS), papillary carcinoma, mucinous carcinoma, medullary carcinoma, metaplastic carcinoma, and a malignant phyllodes tumor. Malignant masses with a cystic component are often characterized by well-circumscribed round, oval, or lobular masses, thereby appearing benign on ultrasonography. On pathology, the cystic component of a malignant mass is identified by cystic degeneration, hemorrhage, necrosis, or ductal dilatation. If the mass is well-circumscribed with a cystic component, a biopsy should be considered in the analysis of the solid component within a mass.
MeSH Terms
Figure
-

Fig. 1 Invasive ductal carcinoma with cystic degeneration. A. Sonography showed a large ill-defined cystic mass (arrow) with a thick septa and a solid nodular component. B. Photography (original magnification, × 12.5; H-E stain) revealed pleomorphic malignant cells and hemorrhagic necrosis (arrow).

Fig. 2 Ductal carcinoma in situ (DCIS). A. Sonography demonstrated multiple conglomerated oval masses within an eccentric cystic component (arrow). B. Photography (original maaagnification, × 40; H-E stain) revealed DCIS of the micropapillary type. The cystic lesions were lined by micropapillary cells and the lumen was filled with necrotic materials (arrow).
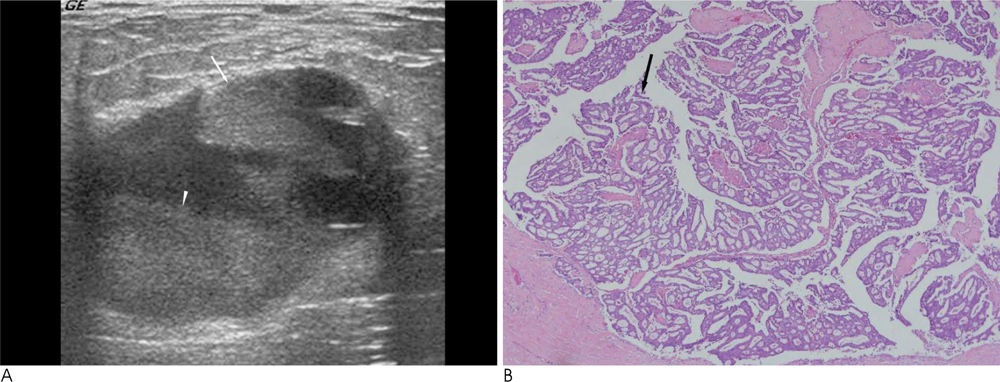
Fig. 3 Papillary carcinoma: aspiration yielded bloody fluid, and following excision biopsy, revealed a low-grade intraductal papillary carcinoma. A. Sonography scan showed a well-circumscribed, oval cystic mass with thick septa and an eccentric solid nodular component (arrow). A fluid-debris level was seen (arrowhead). B. Photography (original magnification, × 100; H-E stain) revealed a dilated duct filled with papillary carcinoma (arrow).

Fig. 4 Mucinous carcinoma. A. Sonography presented a lobulated, oval mass with an eccentric cystic component (arrow). B. Photography (original maaagnification, × 40; H-E stain) revealed malignant cells floating in pools of mucin. The tumor cells were present as small papillary clusters with pleomorphic features. The borders were relatively well circumscribed, and the mucinous pools often mimicked cysts (arrow).

Fig. 5 Medullary carcinoma. A. Sonography showed hypoechoic cystic lesions (arrow) with a smooth and well-circumscribed margined mass. B. Photography (original magnification, × 40; H-E stain) showed medullary carcinoma circumscribing lymphoid tissue with multifocal microcystic degenerations (arrow).

Fig. 6 Metaplastic carcinoma. A. Sonography demonstrated a microlobulated, oval mass with eccentric cystic components (arrow). B. Photography (original magnification, × 40; H-E stain) revealed a metaplastic carcinoma of the breast, which showed spindle and squamoid differentiation. The center of the lesion revealed cystic degeneration by necrosis (arrow).

Fig. 7 Malignant phyllodes tumor. A. Sonography showed a lobulated, oval mass with an eccentric cystic component (arrow). B. Photography (original magnification, × 40; H-E stain) revealed a biphasic tumor composed of cystic epithelial components (arrow) and cellular stroma with marked pleomorphism.
Reference
-
1. Venta LA, Dudiak CM, Salmon CG. Sonographic evaluation of the breast. Radiographics. 1994; 14:29–50.2. Berg WA, Campassi CI, Ioffe OB. Cystic lesions of the breast: sonographic-pathologic correlation. Radiology. 2003; 227:183–191.3. Omori LM, Hisa N, Ohkuma K. Breast masses with mixed cysticsolid sonographic appearance. J Clin Ultrasound. 1993; 21:489–495.4. Harvey JA. Unusual breast cancers: useful clues to expanding the differential diagnosis. Radiology. 2007; 242:683–694.5. Moon WK, Myung JS, Lee YJ, Park IA, Noh DY, Im JG. US of ductal carcinoma in situ. Radiographics. 2002; 22:269–280.6. Wagner AE, Middleton LP, Whitman GJ. Intracystic papillary carcinoma of the breast with invasion. AJR Am J Roentgenol. 2004; 183:1516.7. Lam WW, Chu WC, Tse GM, Ma TK. Sonographic appearance of mucinous carcinoma of the breast. AJR Am J Roentgenol. 2004; 182:1069–1074.8. Liberman L, LaTrenta LR, Samli B, Morris EA, Abramson AF, Dershaw DD. Overdiagnosis of medullary carcinoma: a mammographic-pathologic correlative study. Radiology. 1996; 201:443–446.9. Gunhan-Belgen I, Memis A, Ustun EE, Zeikioglu O, Ozdermir N. Metaplastic carcinoma ot the breast: clinical, mammographic, and sonographic findings with histopathologic correlation. AJR Am J Roentgenol. 2002; 178:1421–1425.10. Liberman L, Bonaccio E, Hamele-Bena D, Abranson AF, Cohn MA, Dershaw DD. Benign and malignant phyllodes tumors: mammographic and sonographic findings. Radiology. 1996; 198:121–124.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Small Breast Cancer (≤ 5 mm): Ultrasonographic Features and Clinical and Pathological Characteristics
- Differentiation of Benign and Malignant Cystic Lesions of the Breast according to Sonographic Findings
- Ultrasonographic Findings of Metaplastic Squamous Breast Carcinoma and the Pathologic Correlation
- Pathologic Evaluation of Breast Cancer after Neoadjuvant Therapy
- Radiologic findings of male breast cancer: two cases report
