J Rheum Dis.
2014 Apr;21(2):82-86. 10.4078/jrd.2014.21.2.82.
A Case of Calcium Pyrophosphate Dihydrate Deposition Disease Associated with Primary Hyperparathyroidism
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Keimyung University Donsan Medical Center, Daegu, Korea.
- 2Department of Rheumatology, Hanyang University Hospital for Rheumatic Diseases, Seoul, Korea. junjb@hanyang.ac.kr
- 3Department of Radiology, Hanyang University Hospital for Rheumatic Diseases, Seoul, Korea.
- 4Department of Pathology, Hanyang University Hospital, Seoul, Korea.
- 5Division of Endoclinology, Department of Internal Medicine, Hanyang University Hospital, Seoul, Korea.
- 6Department of Otolaryngology-Head and Neck Surgery, Hanyang University Hospital, Seoul, Korea.
- 7YTS Rheumatology Clinic, Seoul, Korea.
- KMID: 2094662
- DOI: http://doi.org/10.4078/jrd.2014.21.2.82
Abstract
- Calcium pyrophosphate dihydrate (CPPD) deposition disease is a heterogeneous group of diseases with CPPD crystal deposition. Aging is the most common risk factor for CPPD deposition, followed by osteoarthritis and previous injury. Occasionally, CPPD depositions are associated with familial predisposition and metabolic diseases, including hemochromatosis, primary hyperparathyroidism, hypophosphatasia, and hypomagnesemia. CPPD deposition diseases associated with primary hyperparathyroidism in Koreans have rarely been reported. Thus, we report a case of a relatively young female patient with CPPD deposition disease associated with primary hyperparathyroidism, which was diagnosed through a polarized microscopic examination of the synovial fluid and a subtotal parathyroidectomy.
MeSH Terms
Figure
-

Figure 1. Linear calcifications are seen within the medial and lateral joint space of both knees (A) and the hip joints (B).
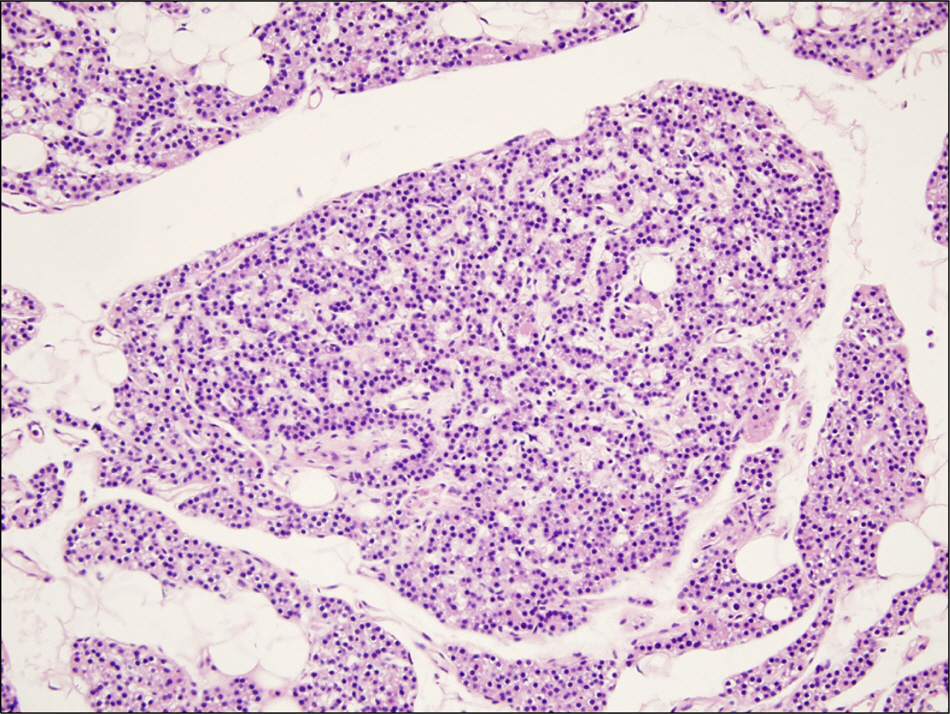
Figure 2. Parathyroid specimen shows chief cell hyperplasia of parathyroid gland (H&E, ×200).
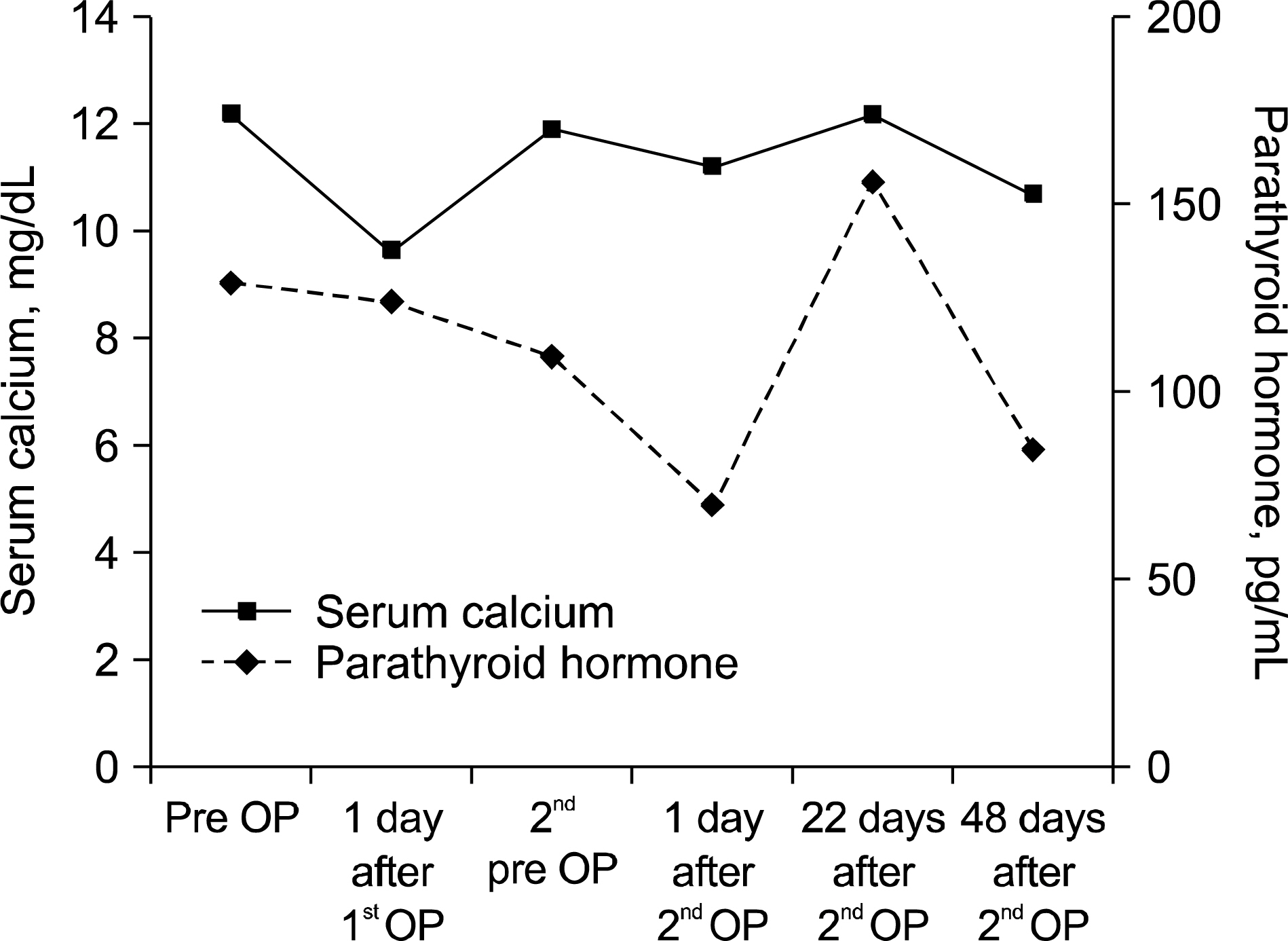
Figure 3. The graph shows the change of serum calcium level and parathyroid hormone level following parathyroidectomy (normal range: 8.4∼10.4 mg/dL, 15∼65 pg/mL, respectively). pre OP: pre-operation.
Reference
-
1. Doherty M, Abhishek A. Calcium pyrophosphate crys-tal-associated arthropathy. Hochberg MC, Silman AJ, Smolen JS, Weinblatt ME, Weisman MH, editors. Rheumatology. 5th ed.p. 1875–87. Philadelphia: Elsevier;2011.
Article2. Salaffi F, De Angelis R, Grassi W. MArche Pain Prevalence; INvestigation Group (MAPPING) study. Prevalence of musculoskeletal conditions in an Italian population sample: results of a regional community-based study. I. The MAPPING study. Clin Exp Rheumatol. 2005; 23:819–28.3. Sanmartí R, Pañella D, Brancós MA, Canela J, Collado A, Brugués J. Prevalence of articular chondrocalcinosis in elderly subjects in a rural area of Catalonia. Ann Rheum Dis. 1993; 52:418–22.4. Terkeltaub R. Calcium crystal disease: calcium pyrophosphate and basic calcium phosphate. Firestein GS, Budd RC, Gabriel SE, McInnes IB, O'Dell JR, editors. Kelly's textbook of rheumatology. 9th ed.p. 1576–96. Philadelphia: Saunders;2012.5. Zhang W, Doherty M, Bardin T, Barskova V, Guerne PA, Jansen TL, et al. European League Against Rheumatism recommendations for calcium pyrophosphate deposition. Part I: terminology and diagnosis. Ann Rheum Dis. 2011; 70:563–70.
Article6. Jeon CH, Choe WH, Ahn JK, Koh JH, Cha HS, Ahn JM, et al. Calcium Pyrophosphate Dihydrate (CPPD) crystal deposition disease mimicking meningitis: a case report and review of the literature. J Korean Rheum Assoc. 2001; 8:134–9.7. Choi ES, Park KJ, Kim YM, Kim DS, Shon HC, Cho BK, et al. Idiopathic Calcium Pyrophosphate Dihydrate (CPPD) crystal deposition disease in a young female patient: a case report. J Korean Shoulder Elbow Soc. 2009; 12:84–8.8. Juhng H, Lee SS, Kim YA. A case of calcium pyrophosphate dihydrate crystal deposition disease associated with gout. J Korean Rheum Assoc. 2002; 9:146–50.9. Jeong JS, Kim TW, Jeong MJ, Im JY, Park MR, Lee CW. A case of CPPD crystal deposition disease in a patient with rheumatoid arthritis and systemic sclerosis. J Korean Rheum Assoc. 2010; 17:412–6.
Article10. Zhang W, Doherty M, Pascual E, Barskova V, Guerne PA, Jansen TL, et al. EULAR recommendations for calcium pyrophosphate deposition. Part II: management. Ann Rheum Dis. 2011; 70:571–5.
Article11. Lew JI. Current understanding and treatment of primary hyperparathyroidism. Endocrinol Metab. 2011; 26:109–17.
Article12. Jones AC, Chuck AJ, Arie EA, Green DJ, Doherty M. Diseases associated with calcium pyrophosphate deposition disease. Semin Arthritis Rheum. 1992; 22:188–202.
Article13. Yashiro T, Okamoto T, Tanaka R, Ito K, Hara H, Yamashita T, et al. Prevalence of chondrocalcinosis in patients with primary hyperparathyroidism in Japan. Endocrinol Jpn. 1991; 38:457–64.
Article14. Udelsman R. Approach to the patient with persistent or recurrent primary hyperparathyroidism. J Clin Endocrinol Metab. 2011; 96:2950–8.
Article15. Wright GD, Doherty M. Calcium pyrophosphate crystal deposition is not always ‘wear and tear' or aging. Ann Rheum Dis. 1997; 56:586–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Idiopathic Calcium Pyrophosphate Dihydrate (CPPD) Crystal Deposition Disease in a Young Female Patient : A Case Report
- Calcium Pyrophosphate Dihydrate Crystal Deposition Disease (Pseudogout) of the Elbow Presenting as A Tumor-Like Mass
- A Case of CPPD Crystal Deposition Disease in a Patient with Rheumatoid Arthritis and Systemic Sclerosis
- A Case of Calcium Pyrophosphate Dihydrate Crystal Deposition Disease Associated with Gout
- Idiopathic Calcium Pyrophosphate Dihydrate (CPPD) Crystal Deposition Disease in a Young Male Patient: A Case Report
