Development of a Coronary Aneurysm at a Sirolimus-Eluting Stent-Implanted Lesion in a Patient With Churg-Strauss Syndrome
- Affiliations
-
- 1Department of Internal Medicine, Vision 21 Cardiac and Vascular Center, Ilsan Paik Hospital, Goyang, Korea. hmchoi49@naver.com
- 2Department of Rheumatology, Ilsan Paik Hospital, Goyang, Korea.
- 3Department of Radiology, Ilsan Paik Hospital, Goyang, Korea.
- KMID: 2094112
- DOI: http://doi.org/10.4070/kcj.2011.41.9.559
Abstract
- A coronary aneurysm (CA) can occur in sirolimus-eluting stent (SES)-implanted coronary lesions. Although several possible mechanisms have been suggested, the precise pathogenesis of a CA in SES-implanted lesions is still unknown. We report a patient with Churg-Strauss syndrome who underwent successful percutaneous coronary intervention with SES and then experienced a CA in an SES-implanted coronary lesion. We describe the CA characteristics through the use of coronary angiography, coronary 64-multidetector computed tomography, and intravascular ultrasound and discuss the etiological factors for the CA in this patient.
Keyword
MeSH Terms
Figure
-
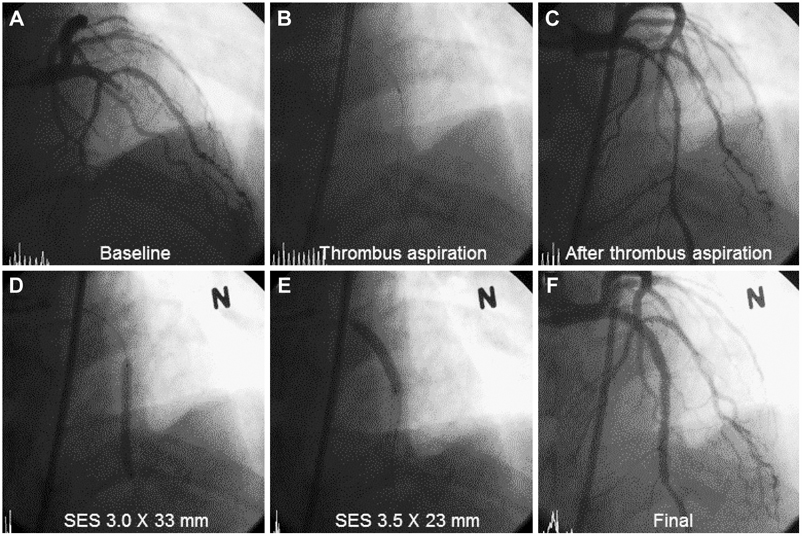
Fig. 1 A: baseline cranial-view coronary angiography (CAG) demonstrated total occlusion of the mid left anterior descending (LAD) artery. B: the manual thrombus aspiration catheter is shown. C: restoration of LAD blood flow after thrombosuction. D and E: two overlapping sirolimus-eluting stents (SES) were implanted from the distal to the proximal LAD artery lesion after balloon dilation. F: final CAG shows the successfully implanted SESs, good thrombolysis, and myocardial infarction flow.
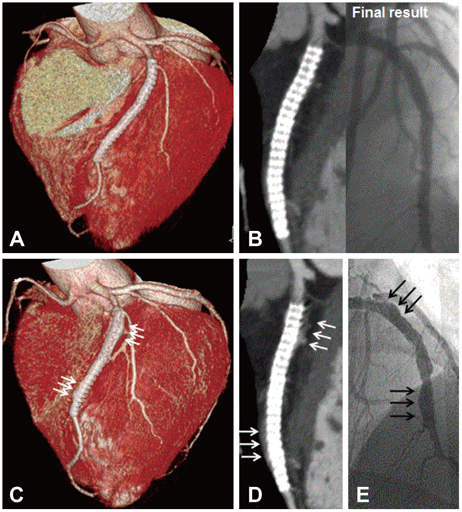
Fig. 2 A and B: a three-dimensional surface reconstruction and volume rendering image view of 64-multidetector computed tomography (MDCT) 14 months after primary percutaneous coronary intervention revealed good configuration of two overlapping sirolimus-eluting stents (SES) and no instent restenosis compared with the final coronary angiography (CAG). C: follow-up three-dimensional surface reconstruction view of coronary 64-MDCT at 39 months revealed diffuse enlargement of the left anterior descending (LAD) artery from the distal to the proximal stent border (triple white arrows). D: volume-rendering image shows crescent-like shaped contrast dye filling out of the stent border with a good configuration of the two overlapping SESs (triple white arrows). E: follow-up CAG shows diffuse multiple conglomeration contrast filling along the stent border without instent restenosis (triple black arrows).
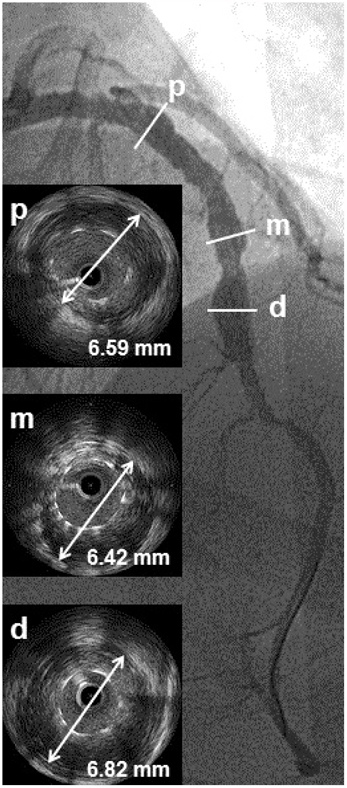
Fig. 3 Intravascular ultrasound assessment revealed a markedly enlarged left anterior descending (LAD) external elastic membrane (EEM) around the sirolimus-eluting stents (SES) struts. Maximal EEM size of the LAD was 6.59 mm at the proximal (p) portion, 6.42 mm at the mid (m) portion, and 6.82 mm at the distal (d) portion.
Reference
-
1. Windecker S, Remondino A, Eberli FR, et al. Sirolimus-eluting and paclitaxel-eluting stents for coronary revascularization. N Engl J Med. 2005. 353:653–662.2. Nienaber CA, Akin I, Schneider S, et al. Clinical outcomes after sirolimus-eluting, paclitaxel-eluting, and bare metal stents (from the first phase of the prospective multicenter German DES.DE registry). Am J Cardiol. 2009. 104:1362–1369.3. Daemen J, Wenaweser P, Tsuchida K, et al. Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: data from a large two-institutional cohort study. Lancet. 2007. 369:667–678.4. Bavry AA, Chiu JH, Jefferson BK, et al. Development of coronary aneurysm after drug-eluting stent implantation. Ann Intern Med. 2007. 146:230–232.5. Mavrogeni S, Manoussakis MN, Karagiorga TC, et al. Detection of coronary artery lesions and myocardial necrosis by magnetic resonance in systemic necrotizing vasculitides. Arthritis Rheum. 2009. 61:1121–1129.6. Masi AT, Hunder GG, Lie JT, et al. The American College of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. 1990. 33:1094–1100.7. Murthy PA, Mohammed TL, Read K, Gilkeson RC, White CS. MDCT of coronary artery aneurysms. AJR Am J Roentgenol. 2005. 184:3 Suppl. S19–S20.8. Alfonso F, Pérez-Vizcayno MJ, Ruiz M, et al. Coronary aneurysms after drug-eluting stent implantation: clinical, angiographic, and intravascular ultrasound findings. J Am Coll Cardiol. 2009. 53:2053–2060.9. Wagner AD, Meyer GP, Rihl M, et al. Acute coronary syndrome associated with Churg-Strauss syndrome. Vasc Health Risk Manag. 2007. 3:775–779.10. Noth I, Strek ME, Leff AR. Churg-Strauss syndrome. Lancet. 2003. 361:587–594.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Coronary Artery Aneurysm after Sirolimus-Eluting Stent Implantation
- Multiple Sequential Complications After Sirolimus-Eluting Stent Implantation: Very Late Stent Thrombosis, Stent Fracture, In-Stent Restenosis, and Peri-Stent Aneurysm
- A Case of Huge Coronary Aneurysm After Implantation of a Sirolimus-Eluting Stent
- Very Late Stent Thrombosis Related to Fracture of a Sirolimus-Eluting Stent
- Angiographic spontaneous pseudo-resolution of a coronary artery aneurysm after implantation of a sirolimus-eluting stent
