Multimodality Imaging Can Help to Doubt, Diagnose and Follow-Up Cardiac Mass
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea. choiek17@snu.ac.kr
- 2Cardiovascular Center, Seoul National University Hospital, Seoul, Korea.
- 3Department of Radiology, Seoul National University Hospital, Seoul, Korea.
- KMID: 2094111
- DOI: http://doi.org/10.4070/kcj.2011.41.9.555
Abstract
- Primary cardiac lymphoma is a very rare form of lymphoma primarily or mainly involving the heart, as in the two cases presented in this report. Various imaging modalities, including coronary computed tomography angiography, cardiac magnetic resonance imaging and positron emission tomography were useful for the characterization and diagnosis of cardiac mass. Pathologic confirmation was successful with endomyocardial biopsy under echocardiographic guidance, intra- and extracardiacally. In primary cardiac lymphoma, diagnosis using multiple modalities may be useful for mass characterization, and for response monitoring after chemotherapy.
Keyword
MeSH Terms
Figure
-

Fig. 1 Angiographic and transthoracic echocardiographic findings of cardiac lymphoma at presentation in case 1. A: coronary angiography shows intact right coronary artery (arrows) and AV nodal artery (dotted arrows) without significant stenosis. B: coronary CT angiography shows preservation of the right coronary artery lumen in spite of the mass at the posterior surface and AV groove of the heart (arrowheads). The AV nodal artery was not compromised in both images. C: modified three chamber view by transthoracic echocardiography shows a mass protruding into the right atrium and right ventricle cavity (arrows), which was the target for endomyocardial biopsy. RCA: right coronary artery, AVN a.: atrioventricular nodal artery, RA: right atrium, RV: right ventricle, LV: left ventricle.
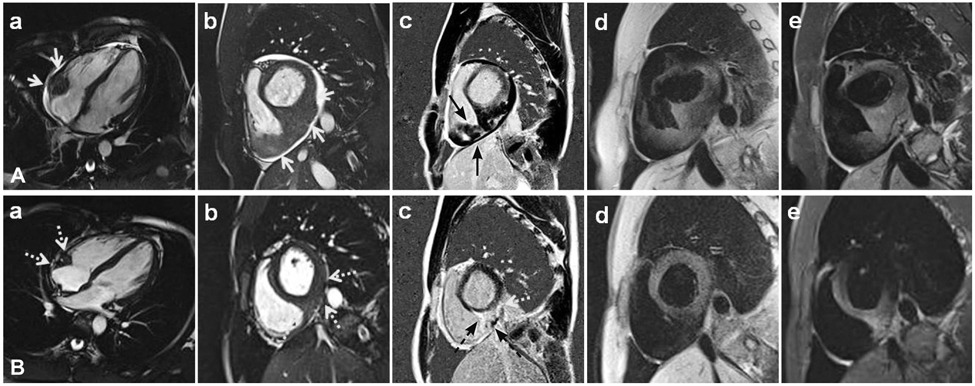
Fig. 2 Cardiac magnetic resonance (CMR) findings of the cardiac lymphoma at presentation (A, upper row) and at follow-up after one cycle of chemotherapy (B, lower row) in case 1. A: iso to slightly high signal intensity mass (arrows) infiltrating the myocardium at the AV groove by steady state free precession (SSFP) image of cardiac MRI (Aa and Ab). Ten-minute delayed MR images with phase-sensitive inversion recovery technique after administration of gadopentetate dimeglumine demonstrated the infiltrative mass (arrows) clearly with heterogeneous enhancement (Ac). B: the mass (dotted arrows) size was markedly reduced after one cycle of chemotherapy in both SSFP (Ba and Bb) and delayed enhancement images with phase-sensitive inversion recovery (Bc). T1 (Ad and Bd) and T2 (Ae and Be) weight images also demonstrate significantly decreased intracardiac mass after chemotherapy.

Fig. 3 Transthoracic echocardiography, chest CT and cardiac magnetic resonance findings of the cardiac lymphoma in case 2. A: subcostal view showing a mass in the right atrium (arrows). B: chest CT image demonstrating a hemogeneously attenuated mass in the right atrium (arrows). C: mass infiltrating the posterior surface of the right atrium (arrows) and interatrial septum (dotted arrows) is demonstrated in steady state free precession (a, b and c), T1 (d) and T2 (e) images.
Reference
-
1. Cairns P, Butany J, Fulop J, Rakowski H, Hassaram S. Cardiac presentation of non-Hodgkin's lymphoma. Arch Pathol Lab Med. 1987. 111:80–83.2. Fujita Y, Ikebuchi M, Tarui S, Irie H. Successful combined treatment of primary cardiac malignant lymphoma with urgent cardiac operation and chemotherapy. Circ J. 2009. 73:967–969.3. Cho SW, Kang YJ, Kim TH, et al. Primary cardiac lymphoma presenting with atrioventricular block. Korean Circ J. 2010. 40:94–98.4. Chang HJ, Kang SM, Rim SJ, et al. A case reort of primary cardiac lymphoma: diagnosis by transverous biopsy under transesophaged echocardiographic guidance. Korean Circ J. 1999. 29:828–832.5. Soslow RA, Baergen RN, Warnke RA. B-lineage lymphoblastic lymphoma is a clinicopathologic entity distinct from other histologically similar aggressive lymphomas with blastic morphology. Cancer. 1999. 85:2648–2654.6. Patel J, Sheppard MN. Primary cardiac T-cell lymphoma in a child. Eur Heart J. 2009. 30:2713.7. Werner D, Schmeisser A, Daniel WG. Images in cardiology: primary cardiac lymphoblastic T cell lymphoma. Heart. 2001. 86:618.8. Abramowitz Y, Hiller N, Perlman G, et al. The diagnosis of primary cardiac lymphoma by right heart catheterization and biopsy using fluoroscopic and transthoracic echocardiographic guidance. Int J Cardiol. 2007. 118:e39–e40.9. Higo T, Takemoto M, Ogawa K, et al. Intracardiac echocardiography-guided cardiac tumor biopsy. Circ J. 2009. 73:381–383.10. Hoey ET, Mankad K, Puppala S, Gopalan D, Sivananthan MU. MRI and CT appearances of cardiac tumours in adults. Clin Radiol. 2009. 64:1214–1230.11. Mariani JA, Dawson MA, Avery S, Taylor AJ. Primary cardiac lymphoma. J Am Coll Cardiol. 2010. 55:e23.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multi Modality Imaging Features of Cardiac Myxoma
- Unusual Presentation Chronic Pulmonary Embolism due to Calcified Right Ventricular Mass
- Aortic Coarctation Following Aortic Valve Replacement: Problem Solving with Multimodality Cardiac Imaging
- FDG-PET in Multimodality Assessment of Cardiac Myxoma
- Assessment of Right Ventricular Function in Pulmonary Hypertension with Multimodality Imaging
