Spontaneous Rupture of Thymic Neuroendocrine Carcinoma: A Case Report
- Affiliations
-
- 1Department of Radiology, Hallym University College of Medicine, Chuncheon, Korea. ijlee2003@medimail.or.kr
- 2Department of Pathology, Hallym University College of Medicine, Chuncheon, Korea.
- KMID: 2079569
- DOI: http://doi.org/10.3348/jksr.2015.73.5.333
Abstract
- Thymic neuroendocrine carcinoma (NEC) is a rare neoplasm with tendencies of local invasion and metastasis. Usually, it is detected incidentally or by its symptoms caused by mass effect. Rupture of the tumor is extremely rare. In this study, we report a case of a ruptured thymic NEC that was combined with a potentially fatal hemorrhage. This lesion was manifested as a progressive bulging of the right cardiac border on serial chest radiographs, and on CT as a large anterior mediastinal mass with heterogeneous enhancement, internal necrosis, and hematoma.
MeSH Terms
Figure
-
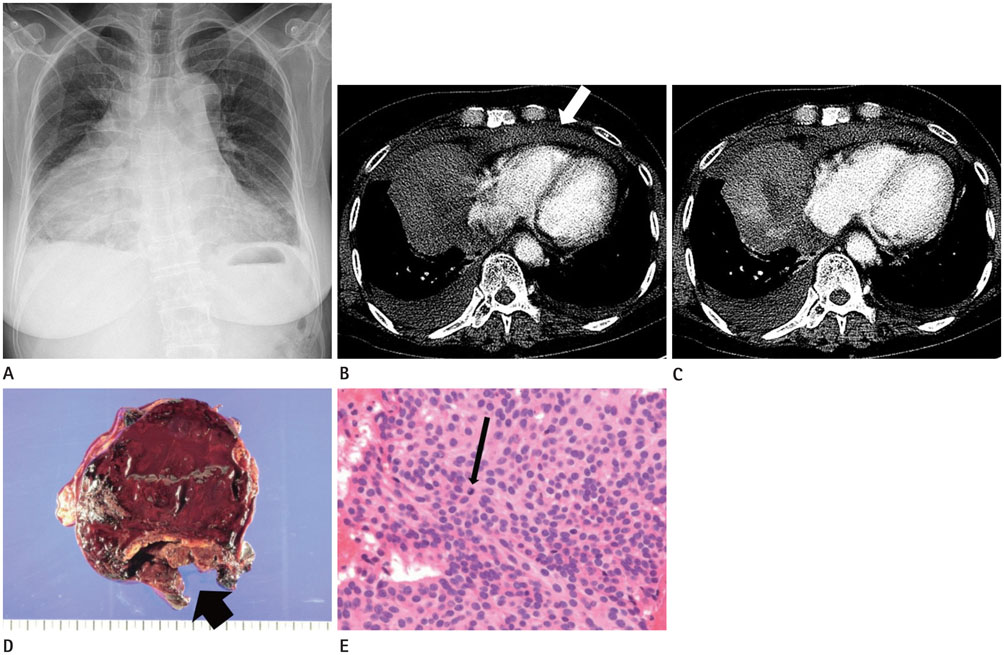
Fig. 1 A 70-year-old woman with ruptured thymic neuroendocrine carcinoma (NEC). A. Initial chest radiograph reveals abrupt increment of right cardiac border bulging with mediastinal widening, compared with previous radiograph (not shown). B. Pulmonary arterial phase of initial triphasic chest CT. There is a large heterogeneous anterior mediastinal mass associated with hemomediastinum (arrow) and bilateral hemothorax. Note that there is no demonstrable enhancement within the tumor. C. In the delayed phase of the initial triphasic chest CT, an irregular enhancement adjacent to the low-density portion of the tumor is noted. D. The cut surface of the tumor shows diffuse hemorrhagic necrosis with foci of viable soft tissue adjacent to the rupture site (thick arrow). E. Histopathological examination for the viable portion of the tumor (hematoxylin and eosin, × 400) shows cells with rounded nuclei and salt-and-pepper chromatin, which are compatible with NEC. A few mitoses are also identified (thin arrow).
Reference
-
1. Chaer R, Massad MG, Evans A, Snow NJ, Geha AS. Primary neuroendocrine tumors of the thymus. Ann Thorac Surg. 2002; 74:1733–1740.2. Fukai I, Masaoka A, Fujii Y, Yamakawa Y, Yokoyama T, Murase T, et al. Thymic neuroendocrine tumor (thymic carcinoid): a clinicopathologic study in 15 patients. Ann Thorac Surg. 1999; 67:208–211.3. Gaude GS, Hattiholi V, Malur PR, Hattiholi J. Primary neuroendocrine carcinoma of the thymus. Niger Med J. 2013; 54:68–71.4. Li H, Wang DL, Liu XW, Geng ZJ, Xie CM. Computed tomography characterization of neuroendocrine tumors of the thymus can aid identification and treatment. Acta Radiol. 2013; 54:175–180.5. Xiang ZM, Liang CM, Ye HM, Tan LL, Hu YS, Zhou YF. [CT manifestations of the thymic carcinoid and literature review]. Nan Fang Yi Ke Da Xue Xue Bao. 2010; 30:557–559.6. Soga J, Yakuwa Y, Osaka M. Evaluation of 342 cases of mediastinal/thymic carcinoids collected from literature: a comparative study between typical carcinoids and atypical varieties. Ann Thorac Cardiovasc Surg. 1999; 5:285–292.7. Katsura H, Iuchi K, Matsumura A, Sueki H, Tanaka H, Ohmori K, et al. A case of rupture of thymic carcinoid. J Jpn Assoc Thor Surg. 2001; 15:764–768.8. Santoprete S, Ragusa M, Urbani M, Puma F. Shock induced by spontaneous rupture of a giant thymoma. Ann Thorac Surg. 2007; 83:1526–1528.9. Ellison RT 3rd, Corrao WM, Fox MJ, Braman SS. Spontaneous mediastinal hemorrhage in patients on chronic hemodialysis. Ann Intern Med. 1981; 95:704–706.10. Choi SJ, Lee JS, Song KS, Lim TH. Mediastinal teratoma: CT differentiation of ruptured and unruptured tumors. AJR Am J Roentgenol. 1998; 171:591–594.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Thymic Neuroendocrine Tumor Associated with Cushing's Syndrome: case report
- 2 Cases of Ectopic ACTH Syndrome due to Thymic Neuroendocrine Carcinoma Associated with Different Clinical Manifestations
- Postoperative Radiotherapy in Thymic Carcinoma : A case report
- Thymic Neuroendocrine Tumor
- A Case of Cutaneous Matestasis Originating from Thymic Carcinoma
