A successful pregnancy in patient with pulmonary hypertension associated with systemic lupus erythematosus
- Affiliations
-
- 1Department of Obstetrics and Gynecology, School of Medicine, The Catholic University of Korea, Suwon, Korea. leegsr@catholic.ac.kr
- KMID: 2077962
- DOI: http://doi.org/10.5468/kjog.2010.53.1.63
Abstract
- Pulmonary hypertension is a rare and potentially life-threatening complication of Systemic lupus erythematosus (SLE), and 5 cases has been previously documented in pregnancy. Four cases died after delivery and only one case was alive. We describe the case of a 28-year-old pregnant woman with pulmonary hypertension related to SLE with no previous history of immunologic disease including SLE. Diagnosis was made at 22 weeks of gestation. Medication including prednisolone and hydroxychloroquinone was commenced immediately and continued throughout the pregnancy. On fetal sonogram, the fetal growth was 3~10 percentile and diastolic notch of uterine arteries was noted. However, a healthy baby girl weighing 2,400 g was born in planned vaginal delivery at gestation week 38. There were no postpartum complications.
Keyword
MeSH Terms
Figure
-
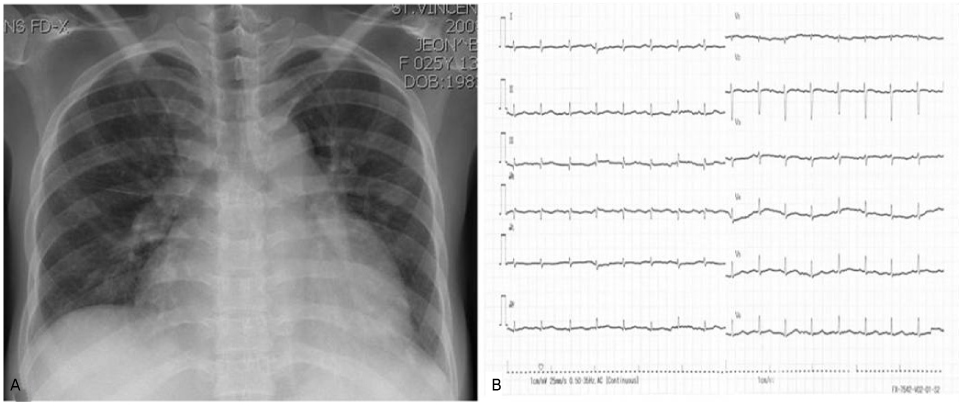
Figure 1 Chest X-ray and Electrocardiogram on admission. Chest X-ray revealed cardiomegaly (cardiothoracic ratio >0.66) and mild pulmonary congestion. Electrocardiogram showed low voltage with normal sinus rhythm.
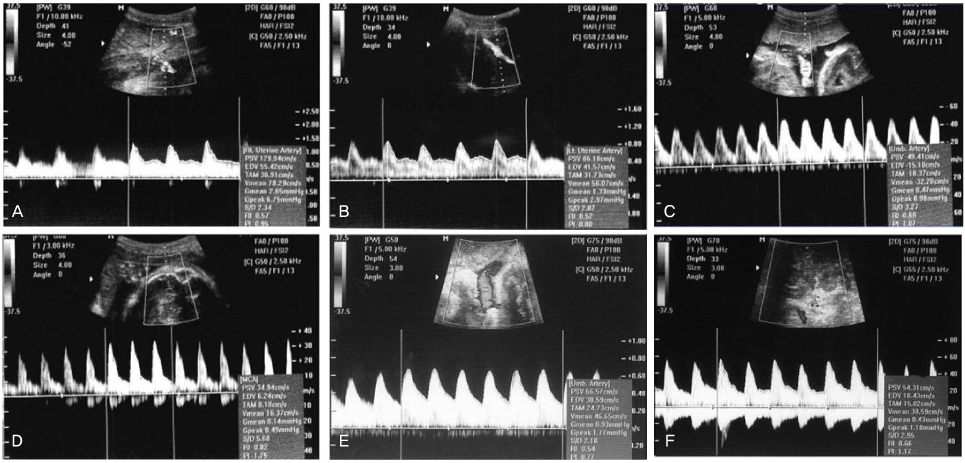
Figure 2 Doppler imaging to evaluate the bilateral uterine artery, MCA and umbilical artery for assessment of fetal health. (A) The early diastolic notching is noted at right uterine artery. (B) The early diastolic notching is noted at left uterine artery. (C) The umbilical artery shows normal velocities at 24 weeks of gestation. RI=0.69. (D) MCA shows high resistance and low diastolic velocities at 24 weeks of gestation. RI=0.82. (E) The umbilical artery shows an increase in diastolic velocities and a decline in RI (=0.54) at 33 weeks of gestation compared as that at 24 weeks of gestation. (F) MCA shows high diastolic velocities at 33 weeks of gestation. R=0.66.
Reference
-
1. McMillan E, Martin WL, Waugh J, Rushton I, Lewis M, Clutton-Brock T, et al. Management of pregnancy in women with pulmonary hypertension secondary to SLE and anti-phospholipid syndrome. Lupus. 2002. 11:392–398.2. Rubin LA, Geran A, Rose TH, Cohen H. A fatal pulmonary complication of lupus in pregnancy. Arthritis Rheum. 1995. 38:710–714.3. Ray J, Sermer M. Systemic lupus erythematosus and pulmonary hypertension during pregnancy: Report of a case fatality. Can J Cardiol. 1996. 12:753–756.4. Haas C. Pulmonary hypertension associated with systemic lupus erythematosus. Bull Acad Natl Med. 2004. 188:985–997. discussion 997.5. Asherson RA, Oakley CM. Pulmonary hypertension and systemic lupus erythematosus. J Rheumatol. 1986. 13:1–5.6. Carmier D, Marchand-Adam S, Diot P, Diot E. Respiratory involvement in systemic lupus erythematosus. Rev Mal Respir. 2008. 25:1289–1303.7. Rubin LJ. Primary pulmonary hypertension. Chest. 1993. 104:236–250.8. Weiss BM, Zemp L, Seifert B, Hess OM. Outcome of pulmonary vascular disease in pregnancy: A systematic overview from 1978 through 1996. J Am Coll Cardiol. 1998. 31:1650–1657.9. Wagenvoort CA, Wagenvoort N. Pathology of pulmonary hypertension. 1977. New York: Wiley.10. Rubin LJ. Approach to the diagnosis and treatment of pulmonary hypertension. Chest. 1989. 96:659–664.11. Aggarwal N, Sawhney H, Vasishta K, Chopra S, Bambery P. Pregnancy in patients with systemic lupus erythematosus. Aust N Z J Obstet Gynaecol. 1999. 39:28–30.12. Kobayashi N, Yamada H, Kishida T, Kato EH, Ebina Y, Sakuragi N, et al. Hypocomplementemia correlates with intrauterine growth retardation in systemic lupus erythematosus. Am J Reprod Immunol. 1999. 42:153–159.13. Venkat-Raman N, Backos M, Teoh TG, Lo WT, Regan L. Uterine artery doppler in predicting pregnancy outcome in women with antiphospholipid syndrome. Obstet Gynecol. 2001. 98:235–242.14. Koleva R, Chernev T, Karag'ozova Zh, Dimitrova V. Antiphospholipid syndrome and pregnancy. Akush Ginekol (Sofiia). 2004. 43:36–42.15. Seo YS, Choi SJ, Choi SJ. The Korean society of Ultrasound in Obstetrics and Gynecology. Fetal Doppler examination. Sonographic imaging of fetal anomalies. 2009. 2nd ed. Seoul: 90–112.16. Hadlock FP, Harrist RB, Marinez-Poyer J. In utero analysis of fetal growth: a sonographic weight standard. Radiology. 1991. 181:129–133.17. Smedstad KG, Cramb R, Morison DH. Pulmonary hypertension and pregnancy: A series of eight cases. Can J Anaesth. 1994. 41:502–512.18. Yin N, Kaestle S, Yin J, Hentschel T, Pries AR, Kuppe H, et al. Inhaled nitric oxide versus aerosolized iloprost for the treatment of pulmonary hypertension with left heart disease. Crit Care Med. 2009. 37:980–986.19. Galiè N, Manes A, Branzi A. Prostanoids for pulmonary arterial hypertension. Am J Respir Med. 2003. 2:123–137.20. Bendayan D, Hod M, Oron G, Sagie A, Eidelman L, Shitrit D, et al. Pregnancy outcome in patients with pulmonary arterial hypertension receiving prostacyclin therapy. Obstet Gynecol. 2005. 106(5 Pt 2):1206–1210.21. Lam GK, Stafford RE, Thorp J, Moise KJ Jr, Cairns BA. Inhaled nitric oxide for primary pulmonary hypertension in pregnancy. Obstet Gynecol. 2001. 98(5 Pt 2):895–898.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Systemic Lupus Erythematosus with Severe Pulmonary Hypertension and Pericarditis
- Pulmonary Hemorrhage with Hemoptysis in Systemic Lupus Erythematosis
- Anesthetic management of cesarean delivery of parturient with systemic lupus erythematosus associated with pulmonary arterial hypertension - A case report -
- Pregnancy in patients with systemic lupus erythematosus
- Pulmonary Thromboendarterectomy for Chronic Thromboembolic Pulmonary Hypertension in a Patient with Antiphospholipid Syndrome and Systemic Lupus Erythematosus
