Yonsei Med J.
2014 Nov;55(6):1624-1630. 10.3349/ymj.2014.55.6.1624.
Modeling of Recovery Profiles in Mentally Disabled and Intact Patients after Sevoflurane Anesthesia; A Pharmacodynamic Analysis
- Affiliations
-
- 1Department of Pediatric Dentistry and Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea.
- 2Department of Clinical Pharmacology and Therapeutics/Anesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Neurology, Korea University College of Medicine, Seoul, Korea.
- 4Department of Anesthesiology and Pain Medicine and Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Seoul, Korea. hanesth@yuhs.ac
- KMID: 2070212
- DOI: http://doi.org/10.3349/ymj.2014.55.6.1624
Abstract
- PURPOSE
Mentally disabled patients show different recovery profiles compared to normal patients after general anesthesia. However, the relationship of dose-recovery profiles of mentally disabled patients has never been compared to that of normal patients.
MATERIALS AND METHODS
Twenty patients (10 mentally disabled patients and 10 mentally intact patients) scheduled to dental surgery under general anesthesia was recruited. Sevoflurane was administered to maintain anesthesia during dental treatment. At the end of the surgery, sevoflurane was discontinued. End-tidal sevoflurane and recovery of consciousness (ROC) were recorded after sevoflurane discontinuation. The pharmacodynamic relation between the probability of ROC and end-tidal sevoflurane concentration was analyzed using NONMEM software (version VII).
RESULTS
End-tidal sevoflurane concentration associated with 50% probability of ROC (C50) and gamma value were lower in the mentally disabled patients (C50=0.37 vol %, gamma=16.5 in mentally intact patients, C50=0.19 vol %, gamma=4.58 in mentally disabled patients). Mentality was a significant covariate of C50 for ROC and gamma value to pharmacodynamic model.
CONCLUSION
A sigmoid Emanx model explains the pharmacodynamic relationship between end-tidal sevoflurane concentration and ROC. Mentally disabled patients may recover slower from anesthesia at lower sevoflurane concentration at ROC an compared to normal patients.
Keyword
MeSH Terms
-
*Anesthesia Recovery Period
Anesthesia, Dental/*methods
Anesthesia, General/*methods
Anesthetics, Inhalation/*administration & dosage/pharmacology
Case-Control Studies
Child
Child, Preschool
Consciousness/drug effects
Dental Care for Disabled/*methods
Dose-Response Relationship, Drug
Female
Humans
Male
Mentally Disabled Persons
Methyl Ethers/*administration & dosage/pharmacology
Anesthetics, Inhalation
Methyl Ethers
Figure
-
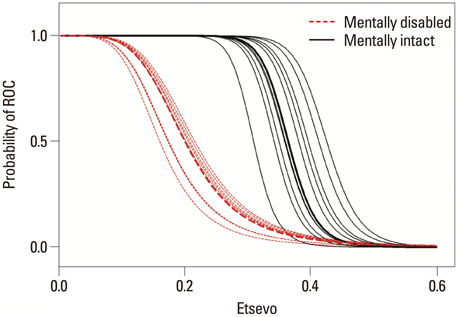
Fig. 1 The relationship between end-tidal sevoflurane concentration and probability of return of consciousness. The red scattered lines indicate individual fits for mentally disabled patients. The black solid lines indicate individual fits for mentally intact patients. The red thick scattered line denotes the representative of fit for mentally disabled patient. The black thick solid line denotes the representative of fit for mentally intact patient. Etsevo, end-tidal sevoflurane concentration; ROC, recovery of consciousness.
Cited by 1 articles
-
How general anesthetics work: from the perspective of reorganized connections within the brain
Teo Jeon Shin, Pil-Jong Kim, Bernard Choi
Korean J Anesthesiol. 2022;75(2):124-138. doi: 10.4097/kja.22078.
Reference
-
1. Larsen B, Seitz A, Larsen R. Recovery of cognitive function after remifentanil-propofol anesthesia: a comparison with desflurane and sevoflurane anesthesia. Anesth Analg. 2000; 90:168–174.
Article2. Escribano-Hernández A, García-Garraus JM, Hernández-García I. Evaluation of satisfaction among relatives of mentally disabled patients who were users of a dental care protocol under general anaesthesia. Med Oral Patol Oral Cir Bucal. 2012; 17:e83–e88.3. Maestre C. The use of general anaesthesia for tooth extraction in young handicapped adults in France. Br Dent J. 1996; 180:297–302.
Article4. Hung WT, Liao SM, Ko WR, Chau MY. Anesthetic management of dental procedures in mentally handicapped patients. Acta Anaesthesiol Sin. 2003; 41:65–70.5. Schraag S, Bothner U, Gajraj R, Kenny GN, Georgieff M. The performance of electroencephalogram bispectral index and auditory evoked potential index to predict loss of consciousness during propofol infusion. Anesth Analg. 1999; 89:1311–1315.
Article6. Nickalls RW, Mapleson WW. Age-related iso-MAC charts for isoflurane, sevoflurane and desflurane in man. Br J Anaesth. 2003; 91:170–174.
Article7. Chernik DA, Gillings D, Laine H, Hendler J, Silver JM, Davidson AB, et al. Validity and reliability of the Observer's Assessment of Alertness/Sedation Scale: study with intravenous midazolam. J Clin Psychopharmacol. 1990; 10:244–251.8. Koo BN, Lee JR, Noh GJ, Lee JH, Kang YR, Han DW. A pharmacodynamic analysis of factors affecting recovery from anesthesia with propofol-remifentanil target controlled infusion. Acta Pharmacol Sin. 2012; 33:1080–1084.
Article9. Lu W, Ramsay JG, Bailey JM. Reliability of pharmacodynamic analysis by logistic regression: mixed-effects modeling. Anesthesiology. 2003; 99:1255–1262.10. Lu W, Bailey JM. Reliability of pharmacodynamic analysis by logistic regression: a computer simulation study. Anesthesiology. 2000; 92:985–992.11. Katoh T, Suguro Y, Ikeda T, Kazama T, Ikeda K. Influence of age on awakening concentrations of sevoflurane and isoflurane. Anesth Analg. 1993; 76:348–352.12. Inomata S, Yaguchi Y, Toyooka H. The effects of clonidine premedication on sevoflurane requirements and anesthetic induction time. Anesth Analg. 1999; 89:204–208.
Article13. Katoh T, Ikeda K. The effects of fentanyl on sevoflurane requirements for loss of consciousness and skin incision. Anesthesiology. 1998; 88:18–24.
Article14. Kihara S, Inomata S, Yaguchi Y, Toyooka H, Baba Y, Kohda Y. The awakening concentration of sevoflurane in children. Anesth Analg. 2000; 91:305–308.
Article15. Cechova S, Zuo Z. Inhibition of glutamate transporters increases the minimum alveolar concentration for isoflurane in rats. Br J Anaesth. 2006; 97:192–195.
Article16. Vadivelu N, Harkness P, Richman S, Shelley KH. Special anesthetic concerns in mentally handicapped institutionalized patients undergoing gynecological procedures in an outpatient setting. Conn Med. 2004; 68:359–362.17. Hwang E, Kim S, Han K, Choi JH. Characterization of phase transition in the thalamocortical system during anesthesia-induced loss of consciousness. PLoS One. 2012; 7:e50580.
Article18. Kroon T, Sierksma MC, Meredith RM. Investigating mechanisms underlying neurodevelopmental phenotypes of autistic and intellectual disability disorders: a perspective. Front Syst Neurosci. 2013; 7:75.
Article19. Purohit BM, Acharya S, Bhat M. Oral health status and treatment needs of children attending special schools in South India: a comparative study. Spec Care Dentist. 2010; 30:235–241.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Application of sevoflurane inhalation sedation in dental treatment: a mini review
- Survey of the sevoflurane sedation status in one provincial dental clinic center for the disabled
- The mentally disabled defendants and the legal procedure
- Employers Attitude for Mentally Disabled People
- The mentally disabled defendants and the legal procedure: An overview and the problems in practice
